Why EGFR Matters in Glioblastoma
When your pathology report comes back after glioblastoma (GBM) surgery, it usually includes a panel of molecular markers. Two of the most commonly flagged are EGFR amplification and a related mutation called EGFRvIII. These are not academic labels. They describe real changes in your tumor's biology, and they increasingly determine eligibility for specific clinical trials and experimental therapies.
This article explains what these alterations are, why they are hard to target, what tests detect them, and what they could mean for your treatment options right now.
To understand your full molecular profile, you may also want to read our overview on Understanding Your GBM Molecular Profile: IDH, MGMT, EGFR & Why They Matter.
What Is EGFR and Why Does Amplification Matter?
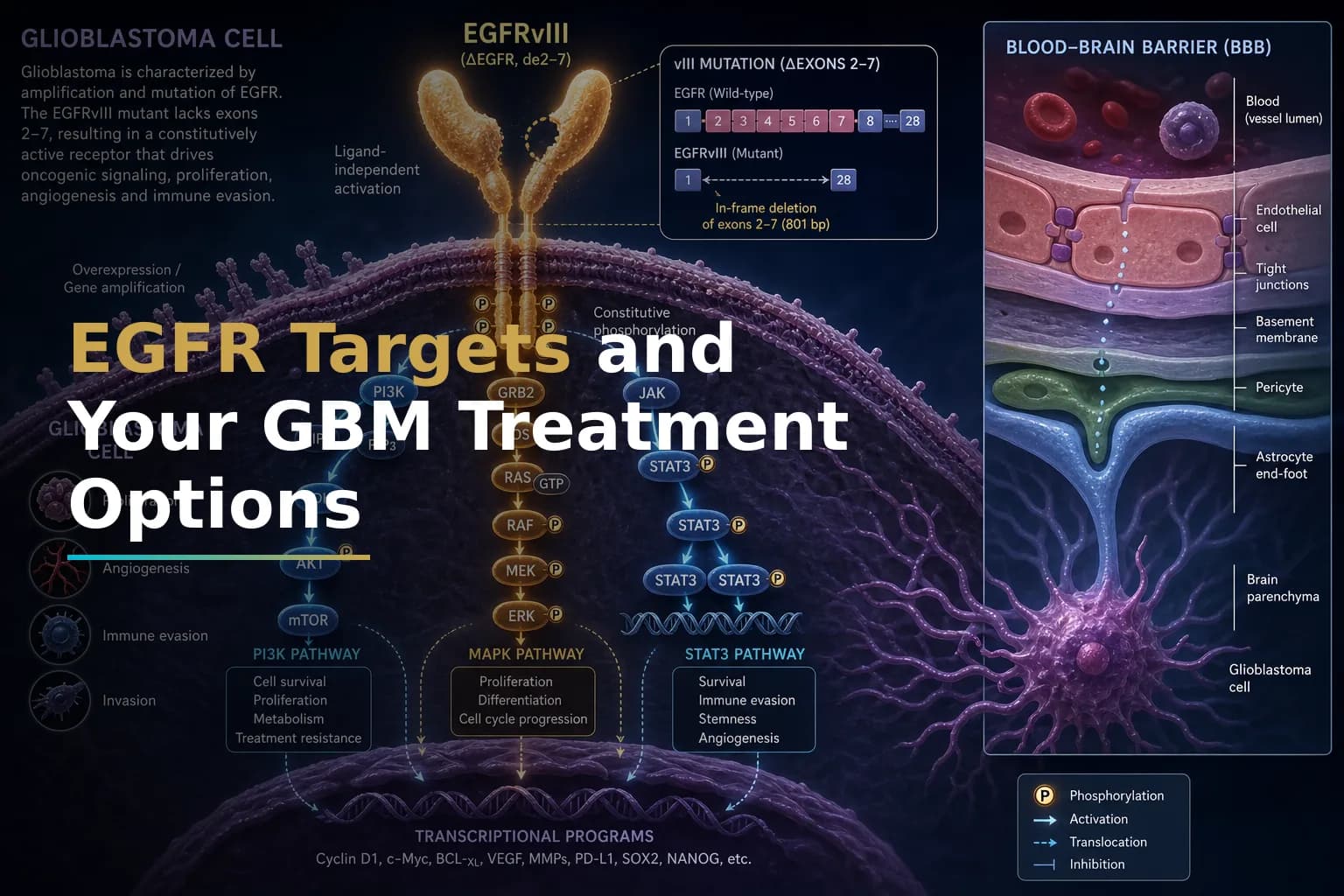
EGFR stands for epidermal growth factor receptor. It is a protein that sits on the surface of cells. In normal tissue, EGFR receives signals from the environment and tells cells when to grow, divide, or repair themselves. It is a tightly controlled system.
In glioblastoma, that control breaks down. Amplification of EGFR means the cell has made many extra copies of the EGFR gene, flooding the cell surface with EGFR proteins. The result is a tumor that sends itself constant "grow" signals, independent of normal checks.
EGFR gene amplification and overexpression occur in about 50% of primary GBMs. Depending on the detection method used, amplification is found in roughly 35–70% of glioblastoma samples, making it one of the most common molecular events in this disease.
Notably, EGFR amplification is found solely in IDH wild-type gliomas and TERT-mutated gliomas, occurring independently of MGMT promoter methylation status. This links EGFR status to the broader molecular identity of your tumor. For more on the TERT connection, see our article on TERT Promoter Mutation in Glioblastoma.
What Is EGFRvIII — and How Is It Different?
EGFRvIII is a mutant version of the EGFR protein. EGFRvIII results from a deletion between exons 2–7 of the EGFR gene, with loss of 267 amino acids from the extracellular domain, creating a constitutively active version of the protein. In plain language: the protein is permanently switched on. It never needs a signal from outside the cell — it just tells the tumor to keep growing.
EGFRvIII appears only in tumors, not in normal brain tissue. EGFRvIII is exclusively expressed on the cell surface of GBMs and other tumors, but it is absent in normal tissues. That tumor-specific presence is what makes it an attractive target for precision therapies — a treatment that recognizes EGFRvIII but ignores healthy cells could limit collateral damage.
EGFRvIII is not present in every EGFR-amplified tumor. Approximately half of tumors with wild-type EGFR amplification express the oncogenic mutant EGFRvIII, which translates to roughly 20–30% of all GBM cases. EGFRvIII preferentially activates the PI3K/Akt signaling pathway, which may contribute to treatment resistance, including resistance to radiation.
How Are EGFR Amplification and EGFRvIII Detected?
Your tumor tissue — usually collected during surgery or biopsy — is the source material for these tests. Several laboratory methods can detect EGFR status:
- Fluorescence in situ hybridization (FISH): FISH is the gold standard for detecting EGFR amplification. It uses fluorescent probes to count gene copies directly under a microscope.
- Next-generation sequencing (NGS): A broader genomic panel that can simultaneously detect EGFR amplification, the EGFRvIII deletion, and hundreds of other alterations in a single test. NGS is increasingly used because of its efficiency and comprehensive scope.
- RT-PCR: A targeted method commonly used to detect the EGFRvIII messenger RNA, which reflects whether the mutant protein is actually being made by tumor cells.
- Immunohistochemistry (IHC): A staining technique that uses antibodies to detect the EGFRvIII protein in tissue sections. Many clinical trial eligibility criteria specifically accept IHC confirmation of EGFRvIII positivity.
One important practical point: EGFRvIII expression may change in a subset of patients at recurrence. A tissue result from your original surgery may not reflect your tumor's biology at the time of recurrence. Most current EGFRvIII-targeted trials require confirmation of EGFRvIII status from the most recent available tumor specimen.
Why Has Targeting EGFR in GBM Been So Difficult?
Given how common EGFR alterations are in GBM, you might expect that EGFR-blocking drugs — which work well in some cancers like non-small-cell lung cancer — would have already made a difference here. So far, that has not been the case.
Targeted therapy with EGFR-tyrosine kinase inhibitors (TKIs) or antibodies has shown only limited efficacy in GBM patients. Researchers have identified several reasons:
- The blood-brain barrier: Most EGFR-targeting antibodies and many small molecules cannot cross from the bloodstream into the brain at useful concentrations. For more on this, see our article on Angiogenesis and Blood-Brain Barrier Disruption in Glioblastoma.
- Downstream pathway mutations: Mutations in signaling molecules downstream of EGFR/EGFRvIII — such as PTEN and NF1 mutations — keep downstream pathways active despite upstream inhibition. Blocking EGFR at the cell surface does not help if the pathway stays active further along the chain.
- Tumor heterogeneity: Different cells within the same tumor may or may not carry EGFR amplification or EGFRvIII. Cells that do not depend on EGFR signaling can survive and repopulate the tumor even after EGFR-targeted treatment.
- Extrachromosomal DNA: EGFR amplicons in GBM often exist outside the main chromosomes, on small circular pieces of DNA. This makes it easier for tumor cells to rapidly shed or gain copies, allowing them to adapt around targeted therapies.
These challenges have pushed researchers toward more complex approaches, including cell therapies, bispecific antibodies, and combination strategies.
Current and Emerging Treatment Strategies That Target EGFR/EGFRvIII
Despite these difficulties, EGFR and EGFRvIII remain among the most actively studied targets in GBM research. Here is a summary of approaches currently in development:
CAR-T Cell Therapy
EGFR is classically amplified in glioblastoma, and the EGFRvIII variant makes it a potential target for CAR-T cell therapy. CAR-T cells are immune cells genetically engineered to recognize and attack EGFRvIII-positive tumor cells.
Early phase clinical trials showed that a Phase I trial confirmed successful on-target activity and significant EGFRvIII antigen reduction in the brain following a single intravenous dose. However, objective responses were inconsistent, and CAR-T cells targeting EGFRvIII face challenges in clinical settings because of antigen loss and uneven expression across the tumor.
Newer designs are addressing these gaps. The CARv3-TEAM-E T Cells trial (NCT05660369) tests a dual-targeting approach that uses EGFRvIII detection to trigger a second attack against wild-type EGFR — a strategy meant to prevent tumors from escaping by losing EGFRvIII. This trial includes arms for both EGFRvIII-positive recurrent GBM and EGFR-amplified (but EGFRvIII-negative) recurrent GBM.
Another trial, NCT07244666, is evaluating a metabolically armed CAR-T cell therapy targeting EGFRvIII for recurrent glioblastoma.
For a closer look at how CAR-T therapy works and where it stands for GBM patients, see our article on CAR-T Cell Therapy for GBM: What Patients Need to Know in 2026.
Bispecific Antibodies
Bispecific antibodies are designed to physically link an EGFRvIII-expressing tumor cell with a T cell, prompting an immune attack. The AMG 596 trial (NCT03296696) studied this approach in EGFRvIII-positive GBM patients, including both newly diagnosed and recurrent cases.
Antibody-Drug Conjugates
Antibody-drug conjugates (ADCs) use an antibody that binds to EGFR as a vehicle to deliver a toxic payload directly into tumor cells. ABT-414 is one such agent studied in clinical trials for EGFR-amplified GBM. The antibody targets a tumor-selective EGFR epitope, meaning it is designed to prefer the overexpressed or mutated form of EGFR found on tumor cells rather than normal tissue.
Peptide Vaccines
Rindopepimut was an EGFRvIII-targeting peptide vaccine that generated significant early interest. It works by training the immune system to recognize the EGFRvIII protein as foreign and mount an attack. A large phase III trial (ACT IV) did not meet its primary endpoint, but researchers learned important lessons about tumor heterogeneity and vaccine timing that are shaping next-generation vaccine designs.
SynNotch Receptor Strategies
A newer approach listed in recent trial updates is the Anti-EGFRvIII synNotch Receptor Induced Anti-EphA2/IL-13Rα2 CAR (E-SYNC) T Cells trial. This Phase I trial tests a logic-gated system: EGFRvIII on the tumor surface first activates the synNotch receptor, which then turns on a CAR targeting two additional antigens. This tiered approach aims to improve precision and reduce off-tumor effects.
How EGFR/EGFRvIII Status Affects Clinical Trial Eligibility
This is where a molecular test result becomes directly actionable. Most trials targeting EGFR or EGFRvIII require tissue-based confirmation before enrollment. In practice, that usually means:
- EGFRvIII positivity confirmed by IHC, PCR, or NGS is a standard inclusion criterion. Many trials will not enroll without this on your pathology report.
- Recurrence confirmation: Most trials require that your tumor has progressed after standard first-line treatment (surgery, radiation, and temozolomide chemotherapy).
- Performance status: A Karnofsky Performance Status (KPS) of 60–70 or above is typically required, reflecting functional independence.
- Steroid dose: Several trials require that patients are off corticosteroids or on a stable, low dose, because steroids can suppress the immune cells these therapies depend on.
- Re-biopsy at recurrence: Some trials now require fresh tumor tissue from the recurrent lesion rather than the original surgical sample, particularly given the known problem of EGFRvIII loss over time.
In patients with recurrent glioblastoma being evaluated for EGFRvIII-directed therapy, EGFRvIII status should be reassessed using recurrent tumor tissue to confirm the target is still present before committing to an EGFRvIII-directed approach.
Also worth knowing: upon tumor recurrence, EGFR amplification status from the primary tumor is generally retained, and the majority of EGFRvIII-positive glioblastomas maintain EGFRvIII positivity at recurrence — though a meaningful minority do not, which is why re-testing matters.
If you are newly diagnosed or recently recurrent, this is a good time to ask your neuro-oncologist whether your molecular profiling report includes EGFR amplification status and an EGFRvIII result. If it does not, ask whether additional testing can be ordered. See our guide on What to Expect in the First 30 Days After Diagnosis for help assembling your diagnostic information.
What If Your Tumor Is EGFR-Amplified but EGFRvIII-Negative?
This is a common situation. You may have EGFR amplification — extra copies of the gene — without the specific EGFRvIII deletion. This does not disqualify you from all EGFR-focused trials. Several trials, including the CARv3-TEAM-E study, now include arms specifically for participants with EGFR amplification but no EGFRvIII mutation, recognizing that wild-type EGFR overexpression is itself a targetable alteration.
Because the EGFR pathway may drive glioblastoma progression regardless of amplification status, researchers are also studying broader EGFR pathway inhibition strategies that do not depend solely on EGFRvIII positivity.
Connecting EGFR Status to the Rest of Your Molecular Profile
No marker exists in isolation. EGFR amplification in GBM is closely linked to:
- IDH wild-type status: EGFR amplification appears almost exclusively in IDH wild-type GBM — the most common and aggressive form. If your tumor has an IDH mutation, EGFR amplification is unlikely to be relevant. See our article on IDH-Mutant Glioma vs. Glioblastoma for why this distinction matters.
- MGMT methylation: EGFRvIII may interact with the DNA mismatch repair system in ways that could influence temozolomide sensitivity in some tumors. Your MGMT and EGFR results are worth reviewing together with your oncologist. Learn more in our article on MGMT Methylation in Glioblastoma.
- TERT promoter mutation: EGFR amplification is strongly associated with TERT promoter mutations in high-grade glioma, and both are hallmarks of the classical molecular subtype of GBM.
Finding an EGFR/EGFRvIII Trial
The best way to find current trials for which your EGFR status may qualify you is through ClinicalTrials.gov. Search using terms like "EGFRvIII glioblastoma" or "EGFR amplification glioblastoma." Filter by study status ("Recruiting"), distance, and age. Print or save the NCT number for any trial that looks relevant and bring it to your next oncology appointment.
You can also ask your neuro-oncologist or a tumor board whether your molecular profile has been reviewed for trial eligibility. Many academic medical centers hold multidisciplinary tumor boards where these questions are discussed directly.
When to Talk to Your Doctor
Ask your neuro-oncologist about EGFR testing if:
- Your pathology report does not include EGFR amplification or EGFRvIII results
- You are approaching recurrence or have already progressed on standard treatment
- You want to know whether your molecular profile qualifies you for a clinical trial
- You had your original biopsy tested but have not had recurrent tissue assessed
Do not make decisions about treatment changes, supplements, or off-label therapies based on this article alone. Molecular markers are only meaningful in the context of your full clinical picture.
This article is for general information and is not a substitute for medical advice. Always consult your oncologist or care team about your specific situation.