What Is the TERT Promoter Mutation?
Every cell in your body carries a gene called TERT — short for telomerase reverse transcriptase. This gene encodes the core component of an enzyme called telomerase. Telomerase has one main job: it rebuilds the protective caps on the ends of chromosomes, called telomeres, so that cells can keep dividing.
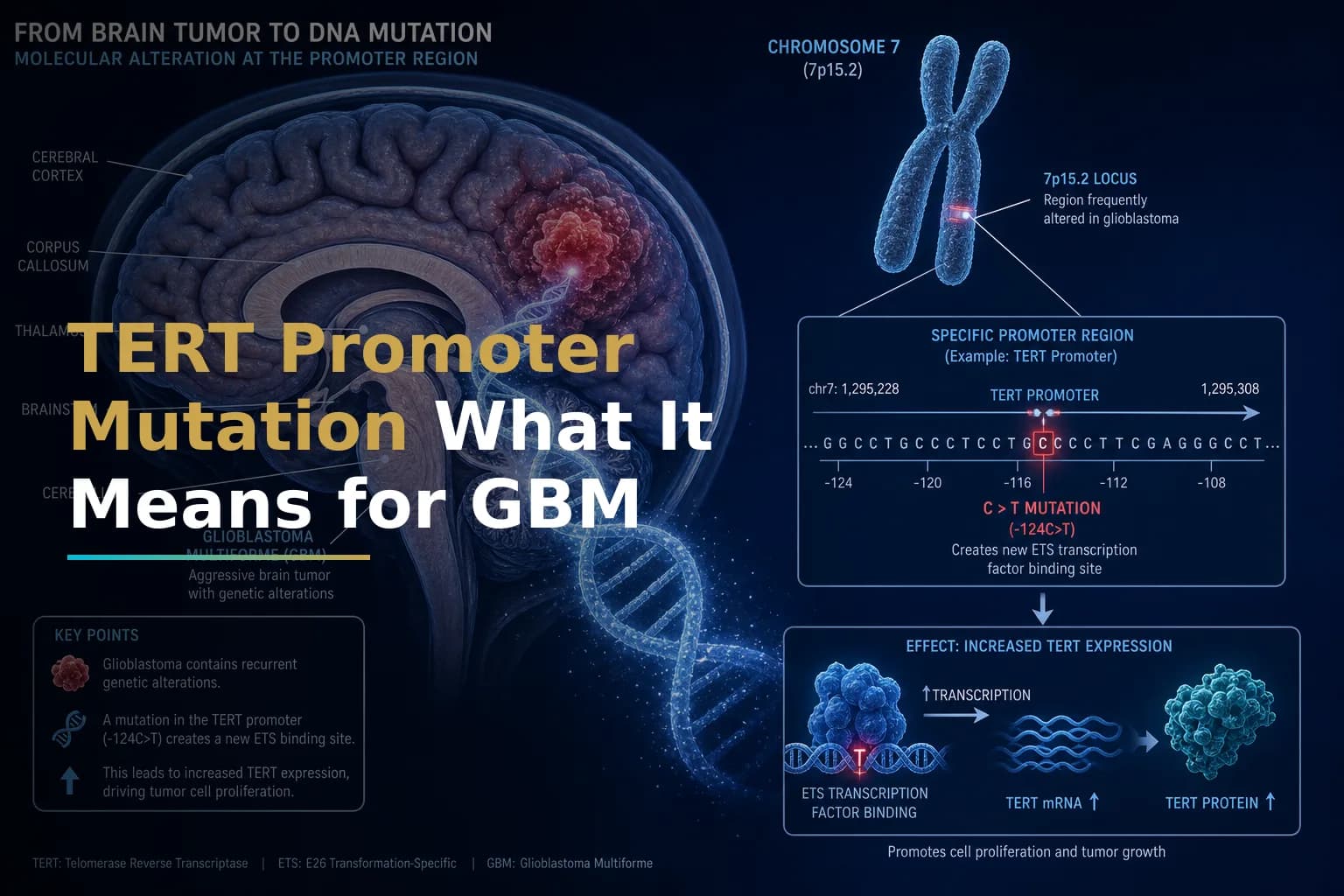
In most healthy adult cells, telomerase is switched off. Cells eventually reach a dividing limit, and that acts as a natural brake on uncontrolled growth. Cancer cells find ways around this brake. In glioblastoma, one of the most common workarounds is a mutation in the promoter region of the TERT gene — the molecular switch that controls when the gene is active.
Research published in PMC shows that two specific mutations — C228T and C250T — are the most common forms of this alteration. These two mutations are mutually exclusive: a tumor carries one or the other, not both. Either mutation increases TERT expression and, as a result, telomerase activity. This is thought to drive tumor growth by helping cancer cells bypass normal aging and replicate without limit.
In plain terms: the mutation flips the TERT switch permanently on, giving glioblastoma cells an indefinite ability to replicate.
How Common Is This Mutation in Glioblastoma?
TERT promoter mutations are very common in glioblastoma. A comprehensive review of telomerase biology in glioblastoma confirmed that TERT promoter mutations are present in up to 80% of glioblastoma samples. They also tend to appear across most or all cancer cells within a single tumor, not just in a small subset.
One study of 304 adult glioblastoma samples found that TERT promoter mutations were present in 66.42% of all adult primary glioblastomas. Other studies report higher rates — particularly among IDH-wildtype tumors, where the range reaches 80–90%.
This makes TERT promoter mutation one of the most common molecular changes seen in this disease. For comparison, it appears in only about 9–20% of lower-grade gliomas such as IDH-mutant astrocytoma.
The 2021 WHO Classification of CNS Tumors formally recognized this. According to published research on TERT detection methods, the 2021 WHO Classification named TERT promoter changes as one of the key molecular markers for classifying CNS tumors — including glioblastoma, oligodendroglioma, and meningioma. If your pathology report lists IDH-wildtype glioblastoma, there is a high probability your tumor carries this mutation.
To learn more about how the full molecular picture is assembled at diagnosis, see our overview: Understanding Your GBM Molecular Profile: IDH, MGMT, EGFR & Why They Matter.
The Biology: How Does This Mutation Drive Tumor Growth?
Understanding the mechanism helps explain why researchers are focused on TERT as a target.
At the molecular level, both the C228T and C250T mutations create an identical 11-base-pair DNA sequence. This sequence forms a new binding site for a family of transcription factors — proteins that switch genes on. The specific protein here is GABPA (GA-binding protein transcription factor), a member of the ETS transcription factor family.
When GABPA binds to this new site, it activates TERT gene transcription. Preclinical research has shown that blocking TERT activity in cancer cells — by reducing the GABPB1L protein — slows growth and weakens the DNA damage response, making glioblastoma cells much more sensitive to standard chemotherapy like temozolomide.
The net result of the mutation is a cycle that keeps tumor cells alive:
- Telomeres are continuously rebuilt, so cancer cells do not age or die on schedule.
- The DNA repair machinery stays active, helping tumor cells survive chemotherapy and radiation.
- An immunosuppressive tumor environment may develop, potentially weakening immune responses.
Because TERT promoter mutations occur early in glioma formation and are spread evenly across tumor cells, they are a particularly appealing therapeutic target — one that is hard for the tumor to escape through selective pressure.
What Does TERT Mutation Mean for Prognosis?
This is where the picture gets more nuanced, and where your oncologist's interpretation of the full molecular panel matters.
On its own, research published in PMC found that patients with TERT promoter mutations without IDH mutations had the worst overall survival. By contrast, tumors carrying both TERT promoter and IDH mutations showed the best overall survival.
This interaction is central to understanding TERT's prognostic role. In IDH-wildtype glioblastoma — the most common GBM subtype — TERT promoter mutation does not confer any benefit. These patients tend to have a more aggressive disease course, and some research has linked TERT-mutant IDH-wildtype GBMs to multifocal or distant spread over time.
A second important interaction involves MGMT promoter methylation. Evidence reviewed in the Nature Index shows that TERT promoter mutations are a negative prognostic marker mainly when paired with an unmethylated MGMT promoter. When MGMT methylation is present, some data suggest it may partially offset the adverse effect of TERT mutation.
Some research also found that in IDH-wildtype GBMs with MGMT promoter methylation, patients with TERT promoter mutations had better survival after standard chemoradiation. The relationship between these two markers is still being studied.
Key takeaway: TERT mutation status does not stand alone. Your neuro-oncologist reads it alongside IDH status, MGMT methylation, EGFR amplification, and other molecular features to form a complete picture. For a closer look at how MGMT methylation fits in, see: MGMT Methylation in Glioblastoma: What This Biomarker Really Means for Temozolomide Response and Your Treatment Plan.
TERT Mutation and the WHO 2021 Classification
Before 2016, glioblastoma diagnosis relied mainly on how tumor tissue looked under a microscope. Since then, molecular biology has changed how these tumors are classified. The 2021 WHO CNS Classification, 5th Edition, now requires molecular data alongside microscopic findings to assign a definitive diagnosis.
For IDH-wildtype glioblastoma, the WHO specifies that the diagnosis can be made when one or more of the following genetic features are present: TERT promoter mutation, EGFR gene amplification, or gain of chromosome 7 combined with loss of chromosome 10. In practice, a tumor previously classified as lower-grade by microscopy alone may now be reclassified as glioblastoma if it carries a TERT promoter mutation — even without classic GBM features like necrosis or abnormal blood vessel growth.
This shift has real consequences. It can mean a more intensive treatment plan, closer follow-up, and different eligibility for clinical trials. If you were recently diagnosed, ask your care team which molecular features drove your specific diagnosis. You can also read more in our guide: Newly Diagnosed Glioblastoma: What to Expect in the First 30 Days After Diagnosis.
For a comparison of IDH-wildtype and IDH-mutant gliomas, see: IDH-Mutant Glioma vs. Glioblastoma: Why Your Diagnosis Type Changes Everything About Treatment and Prognosis.
Current Treatment Implications: Does TERT Status Change What You Receive Today?
At present, TERT promoter mutation status does not directly change the standard treatment regimen for most patients. The Stupp protocol — maximal safe resection followed by concurrent temozolomide and radiation, then adjuvant temozolomide — remains the standard for newly diagnosed glioblastoma regardless of TERT status.
That said, TERT mutation status is increasingly factored into clinical decision-making in a few ways:
- Risk stratification: Oncologists use the combined molecular profile — including TERT, IDH, and MGMT status — to estimate prognosis and guide follow-up intensity. Patients with TERT-mutant, MGMT-unmethylated, IDH-wildtype GBM may be prioritized for aggressive treatment or early clinical trial enrollment given the aggressive nature of this subtype.
- Clinical trial eligibility: Many studies now stratify patients by TERT status or specifically enroll patients whose tumors carry this mutation, since it reliably identifies IDH-wildtype GBM.
- Predictive value in the MGMT context: Emerging data suggest TERT mutation may modify how well patients respond to temozolomide-based chemotherapy, particularly in combination with MGMT methylation status.
To understand how treatment options evolve at recurrence — a common challenge in TERT-mutant, IDH-wildtype GBM — see: Recurrent GBM: Why It Comes Back, What You Can Do, and How to Navigate What Comes Next.
TERT as an Emerging Therapeutic Target
Because TERT promoter mutations are present in nearly all cells of most GBMs, they represent a potentially ideal therapeutic target — unlike mutations confined to only a portion of tumor cells. The goal is to shut off the mechanism that grants cancer cells immortality.
A 2024 systematic review of telomerase-targeted therapies identified several approaches currently under investigation:
- Small-molecule telomerase inhibitors: Drugs designed to block telomerase enzyme activity directly. Preclinical data suggest these may work best when tumor burden is low — for example, after surgical removal and initial chemoradiation.
- GABPB1L inhibition: Because the C228T and C250T mutations work by recruiting the GABP transcription factor complex, researchers are studying whether blocking the GABPB1L protein can selectively suppress TERT activity in tumor cells while leaving normal tissue unaffected.
- Therapeutic vaccines: A clinical trial registered at ClinicalTrials.gov (NCT04280848) is evaluating a telomerase-derived cancer vaccine (UCPVax) in glioblastoma patients. The vaccine aims to trigger immune T-cell responses against the TERT protein, taking advantage of the fact that TERT is broadly expressed in GBM cells but not in normal brain tissue.
- Immunotherapy combinations: Researchers are studying whether TERT mutation status can help predict which patients are most likely to respond to immune checkpoint blockade or other immunotherapy strategies, since the mutation may shape the tumor's immune environment in ways that affect response.
It is important to note that no FDA-approved drug currently targets TERT promoter mutations directly. These approaches are experimental. The only telomerase inhibitor to reach clinical trials — imetelstat — has shown limited efficacy in solid tumors and is currently focused on blood cancers. The research pipeline is active, however, and TERT is a priority target in neuro-oncology drug development.
For a broader look at immunotherapy approaches being studied in GBM, see: The Immunotherapy Landscape in GBM: Beyond Checkpoint Inhibitors.
How Is TERT Mutation Detected?
TERT promoter mutation testing is performed on tumor tissue collected at surgery. The two standard methods are:
- Sanger sequencing: The traditional gold standard. DNA is extracted from the tumor sample and the TERT promoter region is sequenced to identify C228T or C250T substitutions.
- Next-generation sequencing (NGS) panels: Many academic medical centers run comprehensive molecular panels that detect TERT mutations alongside IDH, MGMT, EGFR, and dozens of other relevant alterations in a single test.
An emerging approach is liquid biopsy — detecting TERT mutations in circulating tumor DNA (ctDNA) from a blood sample. Because the C228T and C250T mutations are highly specific to cancer cells, they can theoretically be tracked in the bloodstream over time, offering a non-invasive way to monitor treatment response or catch recurrence earlier. This approach is still largely investigational for GBM but is a growing research area.
Questions to Ask Your Care Team About TERT Mutation
If you or someone you care for has received a glioblastoma diagnosis, these questions can help you have a more informed conversation with your neuro-oncologist:
- Was TERT promoter mutation testing performed on my tumor tissue? What was the result?
- What is my full molecular profile — TERT, IDH, MGMT, EGFR — and how do these results interact to shape my prognosis?
- Are there any current clinical trials enrolling patients based on TERT mutation status?
- Does my TERT status affect my eligibility for any investigational therapies or expanded access programs?
- How will you use my molecular profile to guide surveillance and follow-up?
When to Talk to Your Doctor
If your pathology report mentions TERT promoter mutation — or if you are unsure whether this test was done — bring it up at your next appointment. Molecular profiling is the foundation of modern glioblastoma care, and TERT status is a key part of that picture. If your care team does not include a neuro-oncologist at a high-volume brain tumor center, consider seeking a second opinion or a molecular tumor board review. These resources exist to make sure your treatment plan reflects the most current evidence.
This article is for general information and is not a substitute for medical advice. Always consult your oncologist or care team about your specific situation.