
Radiation therapy for glioblastoma: your complete guide
Understanding every option, every technology, and every decision - written for patients and families, backed by the latest science.
If you or someone you love is facing a glioblastoma diagnosis, radiation therapy is likely part of the conversation. It's completely normal to feel overwhelmed by the number of options and the technical language. This page was built to be your single, trusted resource - everything you need to know, explained in language that respects both your intelligence and your emotional state. You don't need a medical degree to make informed decisions about your care. You just need the right information, presented clearly. That's what this page is for.
Jump to what matters most to you right now:
What it actually is and how it works in glioblastoma
What radiation therapy actually does to cancer cells
Radiation uses high-energy beams (like very focused X-rays, protons, or other particles) to damage the DNA inside glioblastoma cells, making it impossible for them to divide and grow. Cancer cells are more vulnerable to this damage than healthy cells because they divide rapidly and have impaired DNA-repair mechanisms.
Why radiation is essential for glioblastoma
Glioblastoma is an infiltrative tumor - its cells spread beyond the visible tumor margin into surrounding brain tissue. Surgery can remove the bulk of the tumor, but microscopic glioblastoma cells extend into tissue that looks normal on imaging. Radiation targets this invisible margin. Without radiation after surgery, these remaining cells almost always regrow.
The landmark Stupp protocol (2005) - surgery followed by 6 weeks of radiation (60 Gy in 30 fractions) combined with temozolomide chemotherapy - remains the foundation of initial GBM treatment and improved median survival from approximately 12 months to 14.6 months.
The standard radiation course - what to expect day by day
Planning session (simulation)
Usually 1–2 weeks before treatment starts. A custom mask is molded to your face to keep your head perfectly still. A CT scan (and often an MRI) maps the exact treatment area. This session takes about 30–60 minutes.
The mask
The mask can feel claustrophobic and anxiety-inducing for many patients. Most patients find it becomes tolerable after the first few sessions. Some centers allow patients to listen to music, practice breathing exercises beforehand, or request anti-anxiety medication for the first few sessions.
Daily treatment sessions
Typically Monday through Friday for 6 weeks (30 sessions total). Each session lasts about 15–30 minutes, but the actual radiation delivery is only a few minutes. It is painless - you feel nothing during delivery.
Concurrent temozolomide
During radiation, most patients also take temozolomide (an oral chemotherapy pill) daily. This combination is the standard Stupp protocol. After the 6-week course, there's typically a 4-week break before starting maintenance temozolomide cycles.
Hypofractionated schedules - shorter courses for specific situations
Not every patient needs the full 6-week course. For elderly patients (typically 65–70+), patients with poor functional status, or those with large unresectable tumors, shorter courses are available and validated:
40.05 Gy in 15 fractions
3 weeks
with temozolomide - validated by Perry trial (2017)
34 Gy in 10 fractions
2 weeks
25 Gy in 5 fractions
1 week
without temozolomide
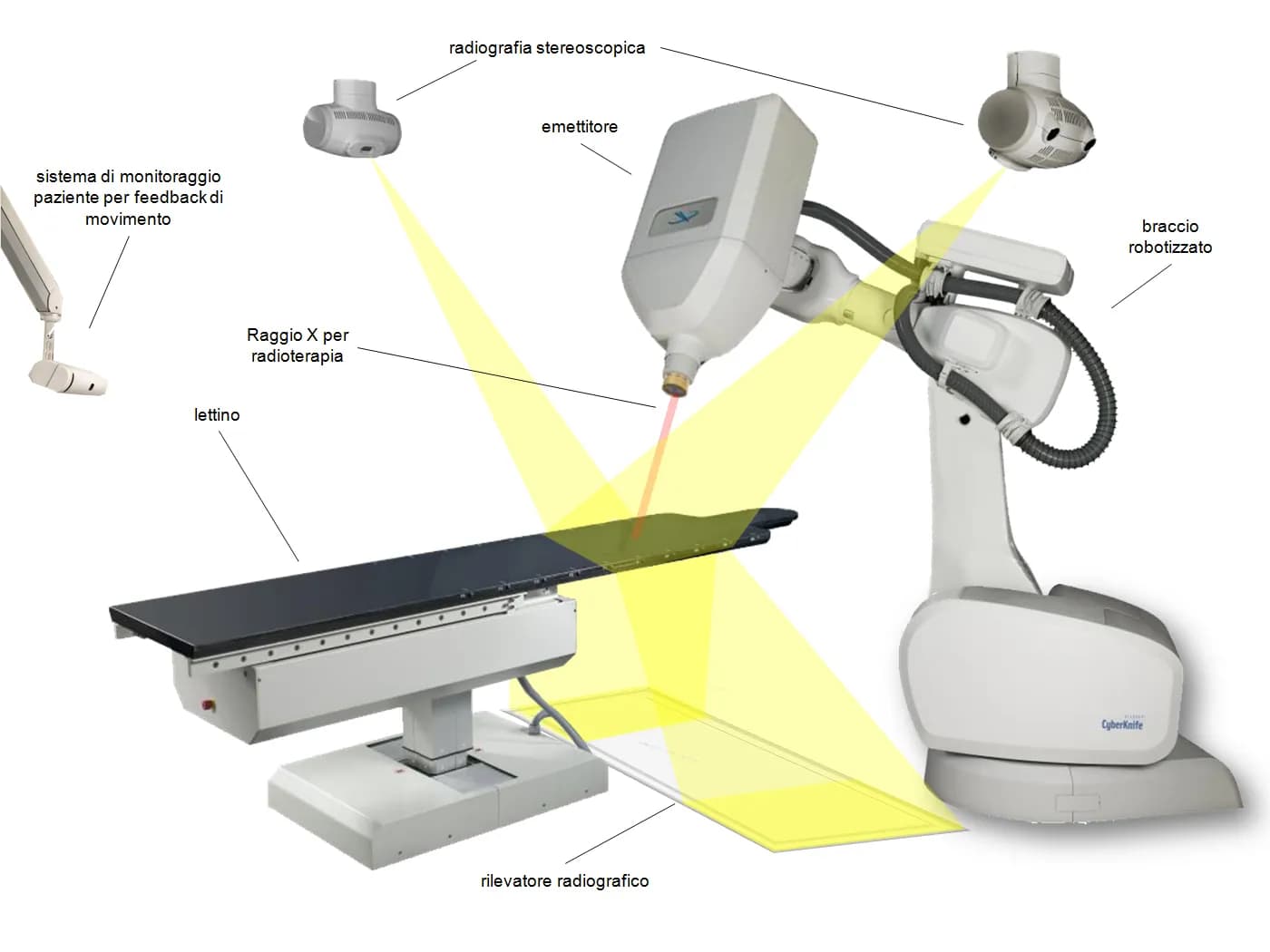
Every radiation platform explained
Not all radiation is the same machine doing the same thing. Different technologies solve different problems. The best choice depends on your specific situation - the size and location of your tumor, whether this is your first radiation course or a re-treatment, your age, your overall health, and what other treatments are in your plan. Here's what each technology does, in plain language.


How your tumor's molecular profile changes the radiation decision
Radiation therapy for glioblastoma is no longer one dose, one schedule, for every patient. Your tumor has a molecular fingerprint - genetic mutations, protein expressions, and epigenetic changes that affect how it responds to radiation. That fingerprint helps your team choose the right radiation strategy, the right dose, and the right combination of treatments.
MGMT methylation
The single most important biomarker for your radiation-chemo plan
MGMT is a DNA repair enzyme - think of it as a repair crew inside your cancer cells. When the MGMT gene promoter is 'methylated' (silenced), the repair crew is disabled, and the cancer cells can't fix the damage caused by temozolomide chemotherapy.
How it changes the radiation decision: MGMT-methylated tumors respond significantly better to combined radiation + temozolomide (median survival ~21.7 months vs. ~12.7 months for unmethylated). For unmethylated tumors, clinical trials like Gliofocus (NCT06388733) and NRG BN007 are testing alternative agents.
Ask your team
"What is my MGMT methylation status? How does it affect whether I should receive temozolomide with radiation, or whether I should consider a clinical trial instead?"
EGFR amplification
A driver of radiation resistance
EGFR (epidermal growth factor receptor) is a protein that tells cells to grow. In about 57% of glioblastomas, the EGFR gene is amplified - producing too much EGFR protein, driving aggressive growth.
How it changes the radiation decision: EGFR amplification activates the PI3K/AKT/mTOR pathway, which promotes cell survival and enhances DNA repair after radiation damage. Your oncologist may consider dose escalation strategies, EGFR-targeted clinical trials, or more aggressive fractionation.
Ask your team
"Does my tumor have EGFR amplification or EGFRvIII? Are there any trials combining radiation with EGFR-targeted therapy?"
PTEN loss
The brake that's missing
PTEN is a tumor suppressor - a molecular 'brake' that normally keeps cell growth in check. In about 40% of glioblastomas, PTEN is mutated or deleted.
How it changes the radiation decision: Without PTEN, the PI3K/AKT/mTOR pathway runs unchecked, promoting radiation resistance. PTEN loss combined with EGFR amplification creates a particularly radiation-resistant profile. Clinical trials targeting this pathway with radiation are underway.
Ask your team
"Does my tumor have PTEN loss? How does this affect my radiation plan?"
p53 status
The guardian under attack
p53 is the 'guardian of the genome' - it detects DNA damage and decides whether the cell should repair itself or self-destruct. In many glioblastomas, p53 is mutated or dysfunctional.
How it changes the radiation decision: When p53 is mutated, the self-destruct mechanism is impaired, and cancer cells may survive radiation damage they shouldn't. However, alternative cell-death pathways can still be triggered - your tumor is not completely resistant.
Ask your team
"What is my tumor's p53 status? Are there strategies to overcome p53-related resistance?"
Tumor hypoxia (HIF-1α)
Why oxygen matters for radiation
The interior of glioblastoma tumors is often hypoxic - meaning it doesn't get enough oxygen. HIF-1α is activated by low oxygen and drives tumor survival in these harsh conditions.
How it changes the radiation decision: Radiation works partly by creating reactive oxygen molecules that damage tumor DNA. In hypoxic areas, there's less oxygen available, making radiation 2–3× less effective. Bevacizumab and novel hypoxia-targeted agents are being explored to address this.
Ask your team
"Is there evidence of hypoxia in my tumor? How might this affect radiation effectiveness?"
IDH status
The molecular dividing line
IDH mutation status is the primary molecular classifier for brain tumors. True 'glioblastoma' is defined as IDH-wildtype by the 2021 WHO classification.
How it changes the radiation decision: IDH-wildtype glioblastomas are generally more radiation-resistant than IDH-mutant tumors. If your pathology shows IDH-wildtype, the treatment strategies on this page apply to you. Always confirm your IDH status with your team.
Ask your team
"What is my IDH status? How does this affect my treatment approach?"
How precision oncology is changing radiation planning
AI-driven radiomics
Researchers are developing AI tools that can predict MGMT methylation status directly from standard MRI scans, potentially eliminating the need for invasive tissue sampling.
Molecular subtype guidance
Glioblastomas fall into subtypes (classical, proneural, mesenchymal) that respond differently to radiation, guiding combination strategies and dose escalation.
Liquid biopsy monitoring
Emerging blood-based tests (circulating tumor DNA) are being explored to monitor tumor response during radiation, allowing treatment adaptation in real time.
Protecting your brain during radiation
One of the biggest fears patients have about brain radiation is what it will do to their thinking, memory, and quality of life. This is a valid concern. Modern radiation planning and supportive care strategies are specifically designed to minimize these effects, and there is real, evidence-based progress in brain protection.
What side effects to expect (and when)
During treatment (weeks 1–6)
Fatigue
The most common side effect. Usually builds gradually and peaks 1–2 weeks after treatment ends. It's not ordinary tiredness - it's a deep, bone-level exhaustion. This is completely normal.
Hair loss
Occurs in the area where beams enter the scalp. Usually temporary, though may be permanent in the highest-dose areas. Begins 2–3 weeks into treatment.
Scalp skin changes
Redness, dryness, itching, or peeling in beam-entry areas. Usually mild with modern techniques.
Nausea
Generally mild with brain radiation. Anti-nausea medications are available.
Headaches & edema
Radiation can cause temporary brain swelling, managed with corticosteroids (dexamethasone). Can cause headaches, worsening neurological deficits, or increased seizure risk.
Early delayed effects (1–6 months after)
Pseudoprogression
In up to 20–30% of GBM patients, MRI scans 2–4 months after radiation show what looks like tumor growth but is actually treatment-related inflammation. This is not true progression. Advanced imaging and rescanning help clinicians differentiate this.
Somnolence syndrome
Some patients experience increased sleepiness 1–3 months after radiation. It's temporary.
Late effects (months to years)
Cognitive changes
Memory, processing speed, attention, and executive function can be affected. Must be distinguished from effects of the tumor itself, steroids, anti-seizure medications, and chemotherapy.
Radiation necrosis
Treated brain tissue can die and swell, occurring in roughly 5–25% of patients. Can mimic tumor recurrence on MRI. Treatable with steroids, bevacizumab, or surgery. Advanced imaging (PET, perfusion MRI, spectroscopy) helps distinguish necrosis from recurrence.
Endocrine effects
If the pituitary gland or hypothalamus receives significant dose, hormonal function can be affected. Periodic endocrine monitoring is recommended.
How your radiation plan protects your brain
Hippocampal sparing
Modern planning deliberately shapes the dose to reduce hippocampal exposure. The NRG CC001 trial showed that hippocampal avoidance + memantine significantly preserved cognitive function.
Organs-at-risk constraints
Radiation plans include strict dose limits for critical structures - brainstem, optic nerves, optic chiasm, cochlea, and hippocampus.
Tight margins with IGRT
Modern image guidance allows tighter margins around the tumor target, meaning less healthy brain in the high-dose zone.
Neuroprotection - what you can do
Memantine
An NMDA-receptor blocker shown to preserve cognitive function when taken during and after brain radiation in a Phase III trial. Ask your oncologist about memantine during radiation.
Cognitive rehabilitation
Working with a neuropsychologist or cognitive rehabilitation specialist. Structured cognitive rehab improves memory, attention, and processing speed.
Physical exercise
Emerging evidence that regular physical activity during and after radiation supports brain health. Even moderate walking has shown benefits.
Sleep hygiene
Prioritizing quality sleep supports brain recovery and cognitive function.
Steroid management
Work with your team to minimize steroid use and taper as soon as medically appropriate - long-term steroids contribute to cognitive issues and other side effects.
Monitoring
Request baseline and periodic neurocognitive testing (before radiation, at 3–6 months, annually) to track changes and intervene early.
Integrative oncology during radiation - evidence-based approaches
Many patients and families ask: "What else can I do alongside radiation to support my body, protect my brain, and potentially improve outcomes?" This is a valid and important question. Integrative oncology combines conventional cancer treatment with evidence-based complementary approaches - not replacing radiation or chemotherapy, but rigorously studied approaches that may work alongside standard treatment.
Ketogenic diet - metabolic support
A high-fat, very-low-carbohydrate diet that may create a metabolic environment less favorable for tumor growth while providing neuroprotective fuel for healthy brain cells. A 2025 Phase 1 trial demonstrated safety and feasibility during standard chemoradiation. A 2025 longitudinal pilot study (72 GBM patients) found those with high adherence to integrative treatment including dietary modification achieved 25.4 months median survival.
Curcumin (from turmeric)
One of the most studied natural compounds in GBM. Curcumin has demonstrated chemotherapy- and radiotherapy-sensitizing properties and crosses the blood-brain barrier. Bioavailability is improved with liposomal curcumin or curcumin with piperine. Clinical doses: 2–8g daily.
Boswellia serrata
Boswellic acids reduce peritumoral edema (brain swelling), potentially serving as a steroid-sparing agent. Multiple studies show reduced edema during and after brain radiation. Clinical dosing: 3,600–4,200 mg standardized extract daily.
Melatonin
Improves sleep quality (critical for brain recovery), has documented antioxidant and neuroprotective properties, and preclinical research suggests direct anti-tumor effects. Clinical protocols use 5–20 mg at bedtime during radiation treatment.
High-dose IV vitamin C
At pharmacological doses (achievable only through IV, not oral), vitamin C generates hydrogen peroxide that selectively damages cancer cells. A Phase II trial at the University of Iowa showed promising results. Patients must be screened for G6PD deficiency.
Exercise during radiation
Structured exercise during brain radiation is safe, and in most cases beneficial. It improves fatigue, mood, cognitive function, and possibly treatment outcomes. Even moderate activity (30 minutes of walking, 3–5 times per week) has measurable benefits.
The Glioblastoma.Center radiation decision framework
At Glioblastoma.Center, we believe the radiation decision should not be made in isolation. It should be the product of four layers of intelligence working together:
Tumor biology
What does your molecular profile (MGMT, IDH, EGFR, PTEN, p53) tell us about how your tumor will respond to radiation? Are there resistance mechanisms we need to account for?
Treatment technology
Given your tumor's size, location, shape, and molecular profile, which radiation platform provides the best geometric and dosimetric match?
Treatment sequencing
How does radiation fit with your surgery, chemotherapy, TTFields, immunotherapy, and clinical trial options? What order maximizes each treatment's contribution?
Whole-patient support
What evidence-based integrative approaches can enhance radiation's effectiveness and protect your brain during treatment?
When glioblastoma comes back
Recurrence is unfortunately common in glioblastoma, and it doesn't mean previous treatment failed - it means the disease is persistent. The good news is that radiation can often be used again, and there are more options and more precision available today than ever before.
Can you get radiation again?
Yes, in many cases. The brain has a cumulative radiation tolerance, but this is not a simple number. It depends on how much time has passed (the brain partially recovers between courses), what area was treated, what dose was given, and how much overlap there would be. The ESTRO-EANO 2024 and 2025 ASTRO guidelines provide specific recommendations.
Re-irradiation decision matrix
| Recurrence Pattern | Preferred Approach | Why This Fits |
|---|---|---|
| Small, focal nodule (< 3 cm), clearly defined, away from prior high-dose area | SRS (single-fraction radiosurgery) | The target is compact and well-defined. SRS delivers a high, effective dose in 1 session with minimal exposure to surrounding brain. |
| Small-moderate recurrence near original treatment field or irregular shape | Fractionated stereotactic radiotherapy (3–5 fractions) | Fractionation allows a biologically effective dose while reducing necrosis risk in previously irradiated tissue. |
| Larger recurrence (> 3 cm) but still localized | Hypofractionated re-irradiation (10–15 fractions) | For larger targets, a single fraction would carry too much necrosis risk. A short course balances tumor control with brain tolerance. |
| Recurrence in an area with very high cumulative dose | Proton-based re-irradiation consultation | Protons may spare surrounding brain that has already been heavily irradiated, reducing toxicity risk. |
| Deep or surgically inaccessible recurrence | Compare LITT vs. SRS vs. fractionated re-irradiation | All local-control tools should be compared - not just radiation - to find the best risk-benefit balance for your specific location. |
| Diffuse, widespread recurrence without a focal target | Re-irradiation may not be the best tool | Systemic therapy, clinical trials, or supportive care may be more appropriate when recurrence is widespread. An honest and important conversation to have with your team. |
Radiation combined with other treatments
Radiation + temozolomide
The Stupp protocol. Temozolomide makes glioblastoma cells more sensitive to radiation. MGMT-methylated tumors benefit most from the combination.
Radiation + tumor treating fields (TTFields/Optune)
The EF-14 trial showed adding TTFields to temozolomide after radiation improved median survival from 16 to 20.9 months. TTFields are typically started after radiation. The TRIDENT trial (NCT04471844) is investigating TTFields with first-line standard of care.
Radiation + immunotherapy
Radiation can cause 'immunogenic cell death' - killing tumor cells in a way that alerts the immune system. Clinical trials are actively exploring combinations with checkpoint inhibitors (nivolumab, pembrolizumab). Reference: NRG BN007 (dual checkpoint blockade for MGMT-unmethylated GBM).
Radiation + bevacizumab
Bevacizumab reduces blood vessel formation and edema. Sometimes combined with re-irradiation at recurrence to reduce edema and potentially improve outcomes.
Sequencing considerations
The order and timing of treatments matters. Surgery before radiation provides tissue for pathology. Radiation during or after chemotherapy creates different synergies. TTFields after radiation avoids interference. Clinical trial eligibility may depend on where you are in the treatment sequence.
Clinical trials in radiation for glioblastoma
Clinical trials aren't a last resort - they're where tomorrow's standard treatments are being built today. Many of the approaches described on this page became available because patients participated in trials.
NRG-BN001 Phase III
The definitive proton vs. photon trial for newly diagnosed GBM, advancing after promising Phase II survival data.
GBM AGILE
An adaptive platform trial testing multiple therapies simultaneously - designed to find answers faster.
NCT04574856
MRI-guided adaptive dose escalation for newly diagnosed GBM.
TRIDENT (NCT04471844)
Investigating TTFields combined with standard first-line therapy.
EF-41 (NCT06556363)
Next-generation TTFields.
LEGATO (NCT04078568)
Re-irradiation trial for recurrent high-grade glioma.
POPCORN
Evaluating proton pulsed reduced dose rate (PRDR) radiotherapy for recurrent high-grade glioma.
Gliofocus (NCT06388733)
Comparing niraparib vs. temozolomide for MGMT-unmethylated GBM.
NRG BN007
Dual immune checkpoint blockade for MGMT-unmethylated newly diagnosed GBM.
BNCT trials
Ongoing in Japan and Finland for recurrent GBM.
Questions to ask your radiation oncologist
Use this as a checklist when preparing for your appointments.
Before starting radiation
- "What type of radiation technique will you use (IMRT, VMAT, proton)? Why is it the best fit for my tumor?"
- "How are you protecting my hippocampus and other critical brain structures in the plan?"
- "Am I a candidate for proton therapy? Would it make a meaningful difference in my plan?"
- "Should I take memantine during radiation to help protect my cognition?"
- "What is the fractionation schedule and why was it chosen for me?"
- "How will you verify my positioning each day (IGRT)?"
- "Are there any clinical trials I should consider for my initial radiation?"
During treatment
- "What side effects should I watch for this week?"
- "Should I be concerned about this level of fatigue?"
- "When should I contact you between appointments?"
After treatment
- "What does my first follow-up MRI show? Could any changes be pseudoprogression?"
- "When should I start neurocognitive monitoring?"
- "What is my cumulative dose record, and can I get a copy for my records?"
About precision oncology & your molecular profile
- "What is my tumor's full molecular profile - IDH, MGMT, EGFR, PTEN status?"
- "How does my MGMT methylation status affect whether temozolomide should accompany radiation?"
- "Does my tumor have any molecular features that suggest radiation resistance?"
- "Should I get comprehensive genomic profiling (Foundation Medicine, Tempus, Caris) if I haven't already?"
- "Are there clinical trials targeting my specific molecular subtype?"
About integrative oncology during radiation
- "Is the ketogenic diet safe and appropriate for me during radiation?"
- "Can I take curcumin or Boswellia during radiation and temozolomide?"
- "Would melatonin be appropriate for me during treatment?"
- "Is there an integrative oncology specialist or dietitian at your center I could consult?"
- "What exercise level is safe for me during radiation treatment?"
- "Are there any supplements I should specifically avoid during radiation?"
If facing recurrence
- "Is re-irradiation an option for my recurrence pattern?"
- "What does my prior dose map show for the area of recurrence?"
- "Should we compare SRS, fractionated re-irradiation, LITT, and proton options?"
- "What clinical trials are available for recurrent GBM in my area?"
- "Are there any centers you'd recommend for a second opinion on re-irradiation planning?"
Why we built this page
We built this page because we believe patients and families deserve more than a one-paragraph description of radiation therapy. You deserve to understand every technology, every trade-off, and every question worth asking - because when you walk into that consultation, knowledge is your greatest tool.
Radiation for glioblastoma is not one plan for every patient. The right approach depends on your tumor's size, location, molecular profile, and treatment history. It depends on whether this is your first course or a re-treatment. It depends on what other therapies are in your plan.
Most importantly, it depends on you - your priorities, your quality of life, and the kind of care you want. We're here to make sure you have everything you need to participate fully in that conversation.
Request a consultation
Let us help you navigate your radiation therapy options.
Request an Appointment
The information on this page is informed by published clinical trials, ASTRO and ESTRO-EANO guidelines, and peer-reviewed research. For detailed references, see our in-depth blog posts on each topic.
This content is for informational purposes only and should not replace professional medical advice. Always consult with your healthcare team about your specific situation.