
Key Takeaways
- Glioblastoma is not one disease. Molecular profiling has revealed that tumors carrying different genetic alterations behave differently and respond differently to treatment.
- The 2021 WHO Classification made molecular markers — not just microscopy — the defining criteria for diagnosis.
- Three markers stand above the rest: IDH mutation status (the first fork in the road), MGMT promoter methylation (your temozolomide predictor), and EGFR amplification (a driver of aggression and gateway to targeted therapies).
- Beyond these three, TERT promoter mutations, PTEN loss, CDKN2A/B deletions, and TP53 mutations increasingly shape prognosis and trial eligibility.
- Every GBM patient should have comprehensive molecular profiling. If it wasn't done at diagnosis, it may still be possible to request it.
Why Molecular Profiling Changed Everything
Until recently, brain tumors were classified almost entirely by how they looked under a microscope. A pathologist would examine cells, note features like cell division rate and abnormal blood vessel growth, and assign a grade. Grade 4 was glioblastoma.
The problem was that two tumors that looked identical under the microscope could behave completely differently. One patient might survive three years; another with a seemingly identical tumor might survive eight months.
That something else turned out to be molecular biology. Large-scale genomic projects like The Cancer Genome Atlas (TCGA) revealed that glioblastoma is not one disease — it is a collection of molecularly distinct diseases that happen to look similar under a microscope.
The 2021 WHO Classification formalized this. For the first time, molecular markers became required for diagnosis. A grade 4 brain tumor with an IDH mutation is no longer called glioblastoma — it's classified as "astrocytoma, IDH-mutant, WHO grade 4," a biologically distinct entity with different prognosis and treatment considerations.
IDH Status: The First Fork in the Road
If there is one molecular marker that matters most, it is your IDH status. IDH (isocitrate dehydrogenase) is an enzyme involved in cellular metabolism. There are two relevant genes: IDH1 and IDH2.
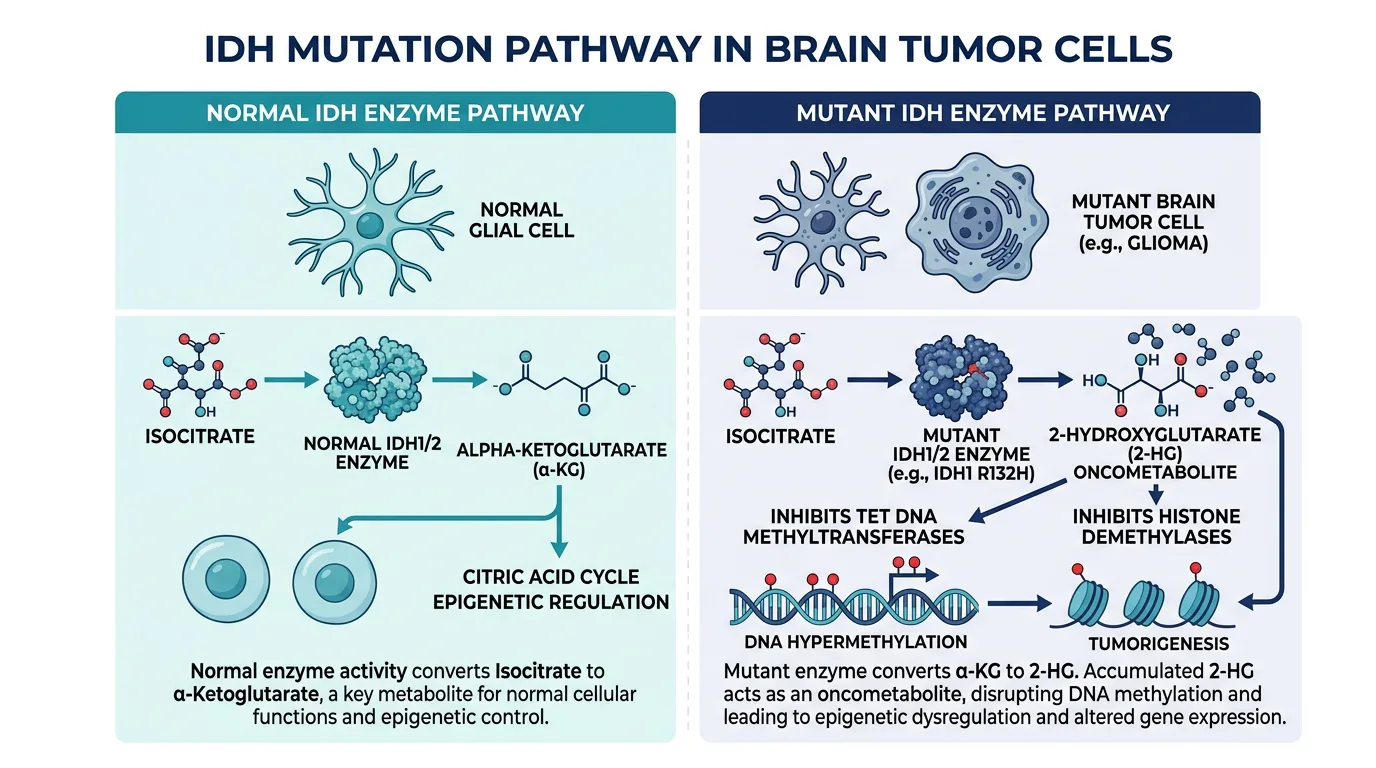
What IDH Mutations Do
In normal cells, IDH enzymes convert isocitrate into alpha-ketoglutarate. When mutated, the enzyme gains an abnormal function: producing an oncometabolite called 2-hydroxyglutarate (2-HG) that disrupts normal gene regulation by interfering with DNA methylation and histone modification.
Here is the critical point: while IDH mutations cause tumors to develop, they paradoxically make those tumors less aggressive than their IDH-wildtype counterparts.
| Subtype | Prevalence | Key Characteristics |
|---|---|---|
| IDH-Wildtype GBM | ~90–95% of glioblastomas in adults | Arises de novo as aggressive, high-grade. Rapid progression, extensive infiltration. Median survival: ~12–15 months. Defined by: no IDH mutation + TERT/EGFR/+7/-10. |
| IDH-Mutant Grade 4 Astrocytoma | Previously "secondary glioblastoma" | Progresses from lower-grade glioma. Younger patients, longer clinical history. Meaningfully better prognosis. No longer called "glioblastoma" (WHO 2021). |
Why IDH Status Matters for Treatment
Vorasidenib (Voranigo) — FDA Approved August 2024: The first FDA-approved targeted therapy for IDH-mutant gliomas in nearly 25 years. In the INDIGO trial, vorasidenib more than doubled progression-free survival (27.7 months vs. 11.1 months). Currently approved for grade 2; trials investigating grade 3–4 use.
Surgical strategy: Research suggests supramaximal resection shows significant survival benefits in IDH-mutant gliomas but more limited impact in IDH-wildtype GBM.
The bottom line: If your report says IDH-wildtype, you have the more common and aggressive form. If IDH-mutant, you have a biologically distinct tumor with emerging targeted therapy options. Either way, IDH status is the foundation for every treatment decision that follows.
MGMT Methylation: Your Temozolomide Predictor
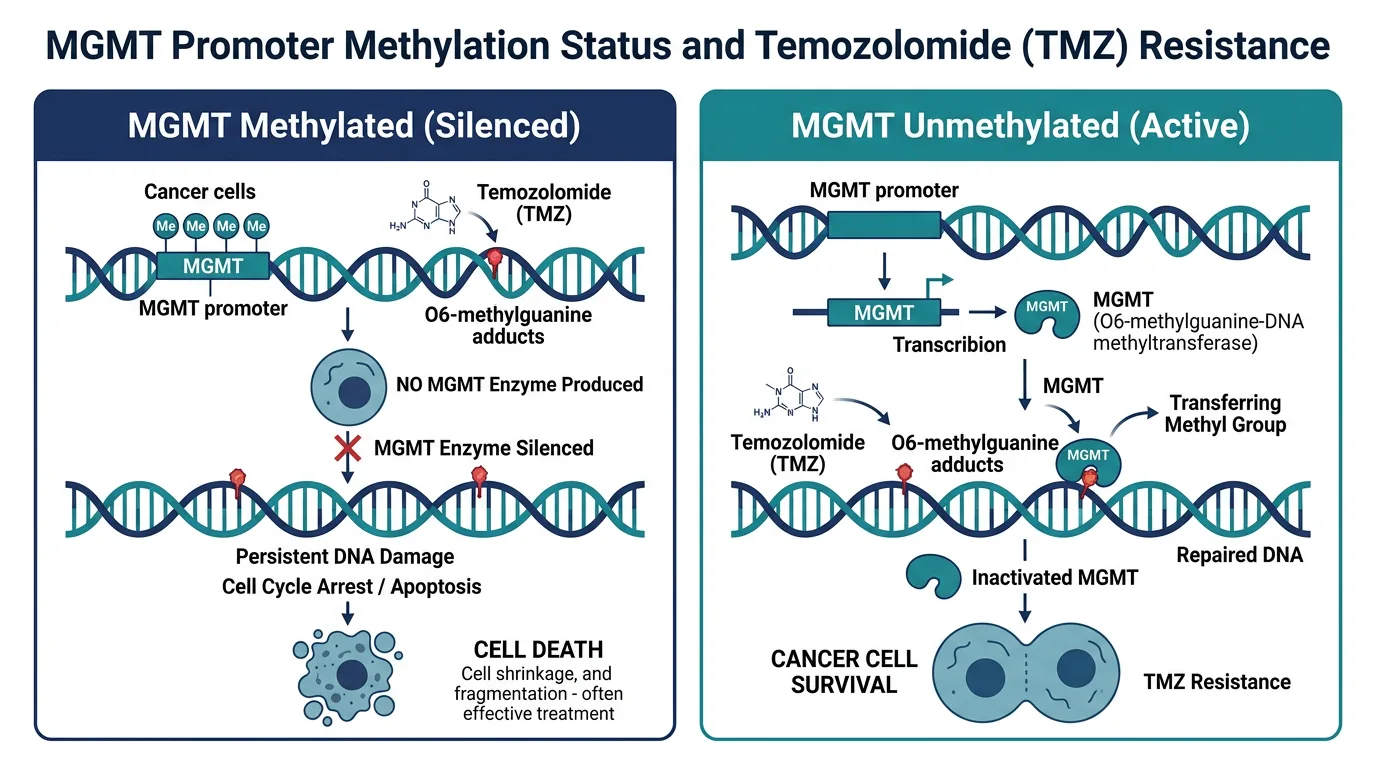
After IDH status, the single most important marker is MGMT promoter methylation status. MGMT is a DNA repair protein whose job is to remove alkyl groups from DNA — specifically the damage that temozolomide creates.
| Status | Prevalence | Key Characteristics |
|---|---|---|
| MGMT Methylated | ~30–35% of GBM patients | MGMT gene silenced → no repair enzyme. Temozolomide damage goes unrepaired. Significantly better TMZ response. Median survival: ~21–23 months. |
| MGMT Unmethylated | ~65–70% of GBM patients | MGMT gene active → produces repair enzyme. Temozolomide damage gets repaired. Limited benefit from standard chemo. Median survival: ~12–15 months. |
The Unmethylated Dilemma
The standard of care was established by the landmark Stupp trial in 2005, but that trial's survival benefit was driven primarily by the methylated subgroup. For unmethylated patients, temozolomide adds modest benefit at best with real side effects.
Emerging Hope: Paxalisib: A PI3K/AKT/mTOR pathway inhibitor that showed a 3.8-month overall survival improvement in newly diagnosed MGMT unmethylated patients (GBM AGILE trial). The FDA has signaled this data could support standard approval. Other approaches: niraparib (PARP inhibitor), combination immunotherapy, TTFields with novel agents.
EGFR: The Proliferation Driver
EGFR is one of the most commonly altered genes in glioblastoma and plays a central role in driving tumor growth, survival, and resistance to treatment.
| Alteration | Prevalence | What It Means |
|---|---|---|
| EGFR Amplification | ~50–60% of IDH-wildtype GBMs | Extra copies of the EGFR gene producing excessive protein. Drives more aggressive behavior and shorter survival. Detected by FISH or next-generation sequencing. |
| EGFRvIII (Variant III) | ~25–30% of EGFR-amplified GBMs | A mutant receptor that is constitutively active — constantly signaling growth without external triggers. Found ONLY on cancer cells, making it an ideal target for CAR-T therapy and targeted antibodies. |
EGFR and immune evasion: Activated EGFR upregulates PD-L1 expression, increases regulatory T cells, and promotes an immunosuppressive metabolic environment — which is why combining EGFR-targeted approaches with immunotherapy is actively being investigated.
Beyond the Big Three: The Expanding Landscape
While IDH, MGMT, and EGFR have the most established clinical impact, additional markers are increasingly influencing prognosis and trial eligibility.
| Marker | Prevalence | What It Means |
|---|---|---|
| TERT Promoter Mutations | 70–80% of IDH-WT GBMs | Activates telomerase, granting tumor cells immortality. One of three markers that can define a GBM diagnosis even without classic histology. |
| PTEN Loss | 30–40% of GBMs | Removes the natural brake on PI3K/AKT/mTOR signaling. Relevant for PI3K pathway inhibitor trials including paxalisib. |
| CDKN2A/B Deletion | Significant % of GBMs | Tumor suppressors for cell cycle control. Homozygous deletion indicates aggressive behavior. Used to upgrade IDH-mutant astrocytomas to grade 4. |
| TP53 Mutations | 30–35% of GBMs | The "guardian of the genome." When mutant, damaged cells continue dividing. Particularly prevalent in IDH-mutant tumors. |
How to Read Your Pathology Report
Your pathology report after surgery or biopsy will contain both histological and molecular findings. Here is what to look for:
| Marker | Result | Method | Impact |
|---|---|---|---|
| IDH1/IDH2 Status | "Wildtype" or "Mutant" | IHC first, sequencing for rare mutations | Determines whether your tumor is glioblastoma (IDH-WT) or astrocytoma grade 4 (IDH-mutant) |
| MGMT Promoter | "Methylated" or "Unmethylated" | MS-PCR or pyrosequencing | Predicts your likely response to temozolomide |
| EGFR | Amplified/Not amplified; EGFRvIII +/- | FISH, NGS, or IHC/PCR | Important for CAR-T and targeted therapy trial eligibility |
| TERT Promoter | Mutated or Wildtype | PCR/sequencing | Relevant for diagnosis and prognosis |
| CDKN2A/B | Deleted or Intact | FISH or NGS | Important for grading and CDK4/6 inhibitor trial eligibility |
| Ki-67 / MIB-1 Index | Percentage (>15–20% = aggressive) | IHC | Indicates how rapidly the tumor is dividing |
If Your Report Is Incomplete: If you're missing key results — particularly IDH, MGMT, and EGFR — ask whether additional testing can be performed on stored tissue. Tissue blocks from your original surgery are often preserved. Comprehensive genomic profiling (FoundationOne CDx, Tempus xT, 4baseCare TarGT) is especially valuable at recurrence when trial eligibility becomes critical.
Matching Your Profile to Treatment and Trials
The era of treating all glioblastomas identically is ending. Your molecular profile increasingly determines which treatments and trials are most likely to benefit you.
- IDH-mutant tumors — Vorasidenib (approved grade 2; trials for 3–4), IDH-targeted combinations, supramaximal resection
- MGMT methylated, IDH-WT — Standard Stupp protocol most beneficial. TTFields add incremental benefit. Strong candidates for combination trials.
- MGMT unmethylated, IDH-WT — TMZ provides limited benefit. Prioritize trials: paxalisib (PI3K), niraparib (PARP), combination immunotherapy.
- EGFR amplified / EGFRvIII+ — Strong candidates for CAR-T trials (Penn, Mass General), EGFR-targeted inhibitors (ERAS-801), antibody-drug conjugates.
- CDKN2A/B deleted — Monitor CDK4/6 inhibitor trials, particularly combining abemaciclib with TTFields.
- PTEN loss — Relevant for PI3K pathway inhibitor trials and metabolic intervention strategies.
What You Should Do With This Information
- Confirm complete molecular profiling — At minimum: IDH, MGMT, EGFR. Ideally add TERT, CDKN2A/B, PTEN, TP53. Pursue comprehensive genomic profiling if available.
- Understand what each result means — Use this guide to frame conversations with your neuro-oncologist. You should understand enough to ask informed questions.
- Use your profile to search for trials — Go to clinicaltrials.gov and filter by your markers. Many trials specify MGMT, EGFR, or IDH status as eligibility criteria.
- Request re-profiling at recurrence — Molecular profiles can shift. EGFR expression can change. If you undergo re-resection, ask that new tissue be profiled.
- Seek a molecular tumor board review — Major centers hold multidisciplinary boards where pathologists, neuro-oncologists, and molecular biologists review complex cases together.
Glossary of Key Terms
| Term | Definition |
|---|---|
| IDH | Metabolic enzyme; mutations produce 2-HG that disrupts gene regulation |
| MGMT | DNA repair enzyme; promoter methylation predicts temozolomide response |
| EGFR | Cell surface receptor driving proliferation; amplified in ~50–60% of IDH-WT GBMs |
| EGFRvIII | Mutant EGFR found only on cancer cells; constitutively active; key CAR-T target |
| TERT | Enzyme maintaining chromosome ends; mutated in ~70–80% of IDH-WT GBMs |
| PTEN | Tumor suppressor that brakes PI3K/AKT/mTOR pathway; lost in ~30–40% of GBMs |
| CDKN2A/B | Tumor suppressors encoding p16/p15; deletion indicates aggressive behavior |
| Methylation | Chemical modification that silences gene expression without changing DNA sequence |
| FISH | Lab technique for detecting gene amplifications or deletions in tumor tissue |
| Vorasidenib | FDA-approved oral inhibitor of mutant IDH1/IDH2 for grade 2 IDH-mutant gliomas |
| Paxalisib | PI3K inhibitor showing activity in MGMT unmethylated GBM (GBM AGILE trial) |
References
- WHO Classification of CNS Tumors, 5th Edition (2021). Louis DN, et al. Neuro-Oncology, 2021; 23(8):1231–1251.
- Stupp R, et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. NEJM, 2005; 352:987–996.
- Mellinghoff IK, et al. Vorasidenib in IDH1- or IDH2-Mutant Low-Grade Glioma (INDIGO Trial). NEJM, 2023; 389(7):589–601.
- FDA Approval Summary: Vorasidenib. Barbato MI, et al. Clinical Cancer Research, 2025; 31(21):4412–4418.
- Vorasidenib clinical advances. Frontiers in Oncology, 2025; 15:1628195.
- Singh S, et al. Glioblastoma at the crossroads. Signal Transduction and Targeted Therapy, 2025; 10:213.
- Molecular markers in GBM prognosis. Cancer Biology & Therapy, 2025.
- Predictive and Prognostic Significance of Molecular Biomarkers in GBM. Biomedicines, 2024; 12(12):2664.
- Cancer Genome Atlas Research Network. Comprehensive genomic characterization. Nature, 2008; 455:1061–1068.
- GBM AGILE Trial. NCT03970447
- MGMT and EGFR characterization in GBM. Neuro-Oncology Advances, 2020.
This article is provided for educational purposes by the glioblastoma.center editorial team. It does not constitute medical advice. Treatment decisions should always be made in consultation with your neuro-oncology team. Molecular profiling capabilities and availability vary by institution.
Last reviewed: March 2026