Key Takeaways
- CAR-T cell therapy re-engineers a patient's own immune cells to recognize and attack glioblastoma — a fundamentally different approach from chemotherapy and radiation.
- In 2025, dual-target CAR-T therapies produced tumor shrinkage in recurrent GBM patients for the first time — something no prior immunotherapy drug had achieved.
- Responses are real but often transient. Durability remains the central unsolved challenge.
- Intracranial delivery (injecting CAR-T cells directly into the brain or CSF) has emerged as safer and more effective than intravenous delivery.
- Multiple clinical trials are actively recruiting. Understanding your tumor's molecular profile — particularly EGFR, EGFRvIII, and IL13Rα2 expression — is essential for eligibility.
Why CAR-T Is Different From Everything Else
If you have been treated for glioblastoma, you are already familiar with the standard playbook: surgery to remove as much tumor as safely possible, radiation therapy, and temozolomide chemotherapy. You may also have used tumor treating fields (TTFields). These remain the foundation of GBM treatment — but they have not fundamentally changed overall survival in two decades.
CAR-T cell therapy represents a completely different category of treatment. Instead of using drugs to poison cancer cells or radiation to damage their DNA, CAR-T therapy turns your own immune system into a precision weapon.
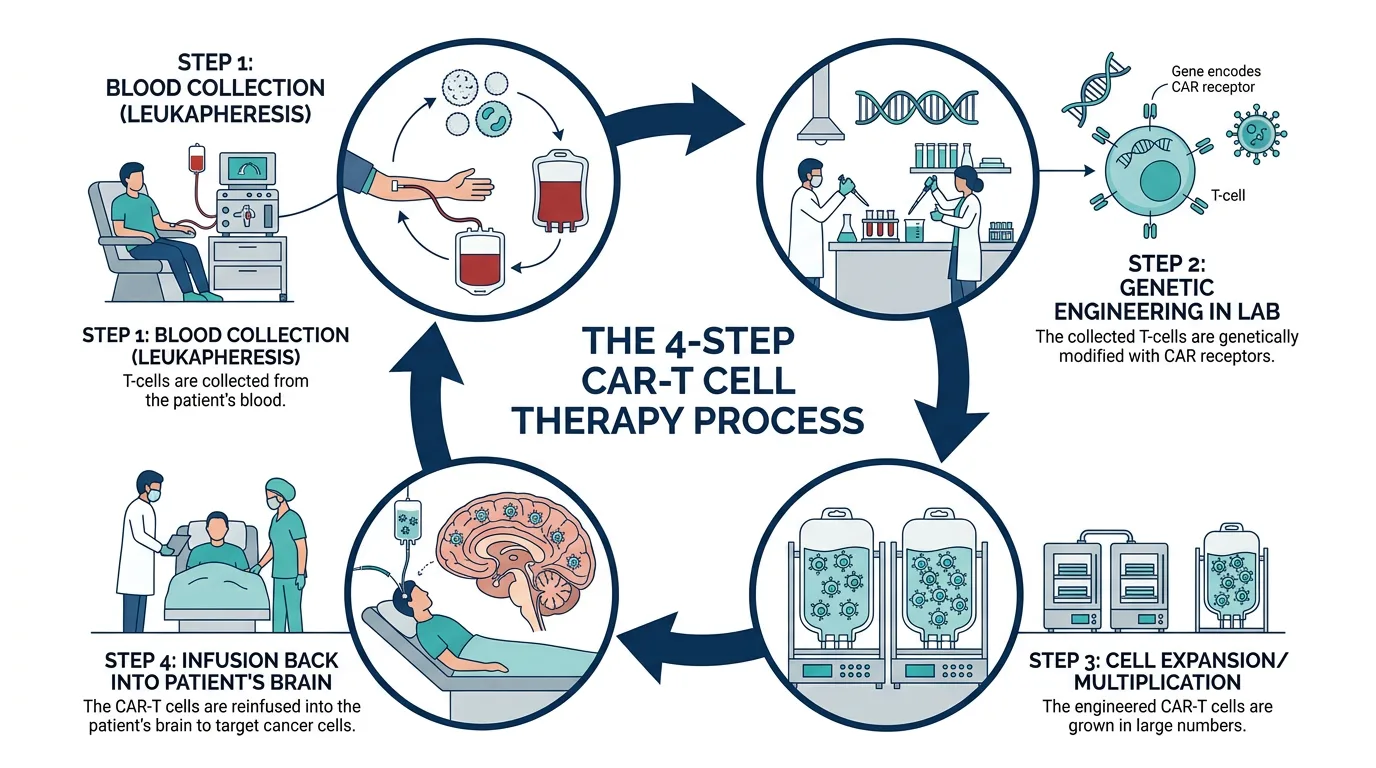
- Collection — T cells are collected from your blood through leukapheresis.
- Engineering — T cells are genetically modified to produce chimeric antigen receptors (CARs) designed to lock onto tumor-specific proteins.
- Expansion — The engineered CAR-T cells are multiplied in a lab to produce millions of copies.
- Infusion — CAR-T cells are infused back — in GBM trials, often delivered directly into the brain through a surgically placed catheter.
CAR-T therapy has already transformed outcomes in blood cancers like certain leukemias and lymphomas. The critical question for the GBM community is whether that success can translate to solid brain tumors — and the honest answer is that we are making real progress, but we are not there yet.
Why GBM Has Been So Hard for CAR-T
GBM is not like a blood cancer. It presents specific biological challenges that have historically defeated immunotherapy approaches:
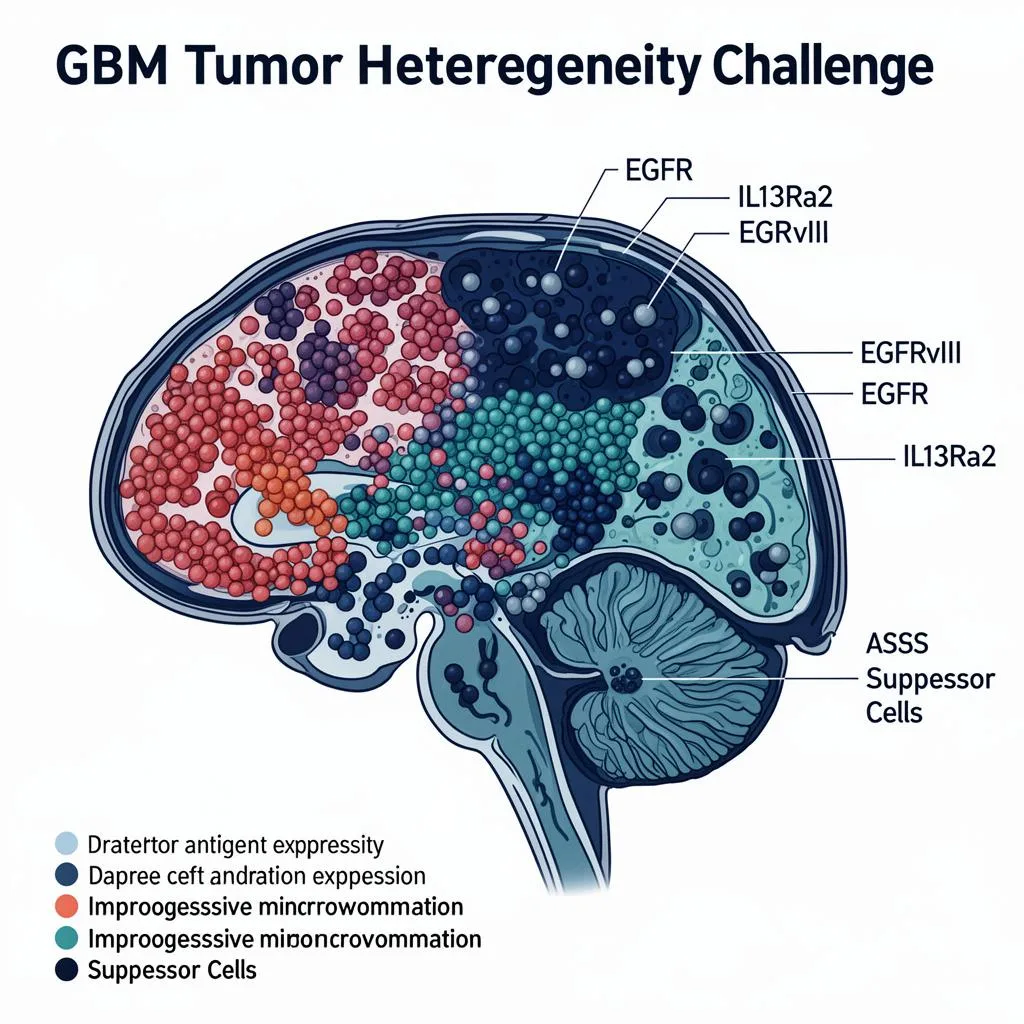
Tumor Heterogeneity
This is the single biggest obstacle. Unlike many blood cancers where virtually every cancer cell displays the same target protein, glioblastoma tumors are composed of mixed populations of cells. If you design a CAR-T cell to target only one protein, the tumor cells that do not express that protein survive and continue growing. This is called antigen escape.
The Immunosuppressive Microenvironment
GBM actively suppresses the immune system in and around the tumor. It recruits regulatory T cells and myeloid-derived suppressor cells that essentially put the brakes on immune responses. Even when CAR-T cells reach the tumor, they enter a hostile environment designed to shut them down.
The Blood-Brain Barrier
The blood-brain barrier controls what enters the brain from the bloodstream. While it protects the brain from toxins, it also blocks many therapies — including immune cells. This is why most GBM CAR-T trials have shifted to intracranial delivery: injecting the cells directly where they need to work.
Low Tumor Mutation Burden
GBM generally has a relatively low tumor mutation burden, giving the immune system fewer obvious targets (neoantigens) to recognize.
The Trials Producing Results Right Now
Three major clinical programs have generated the most significant CAR-T data in GBM through 2025 and into 2026.
Penn Medicine — Dual-Target EGFR + IL13Rα2
Trial ID: NCT05168423
- Targets two proteins simultaneously to address heterogeneity
- 62% tumor shrinkage rate (8 of 13 patients with residual tumor)
- Several patients survived 12+ months (vs. typical 6–10 months for recurrent GBM)
- Next trial will test in newly diagnosed GBM patients
Contact: 1-855-216-0098
Mass General — CAR-TEAM (INCIPIENT Trial)
Trial ID: NCT05660369
- Dual-mechanism: CAR-T targets EGFRvIII + secretes bispecific antibody targeting EGFR
- All 3 initial patients showed dramatic, rapid tumor regression on MRI within days
- Published in The New England Journal of Medicine
- Key limitation: responses are dramatic but often short-lived
Contact: 617-724-6226 | carteamingbm@mgb.org
City of Hope — IL13Rα2-Targeted CAR-T
Trial ID: NCT02208362
- Largest published GBM CAR-T trial: 65 patients treated
- 50% disease-control rate, 23% one-year survival
- One patient achieved 77–100% tumor reduction over 7.5 months
- Higher baseline CD3+ T cells predicted better outcomes
Contact: 626-218-2405
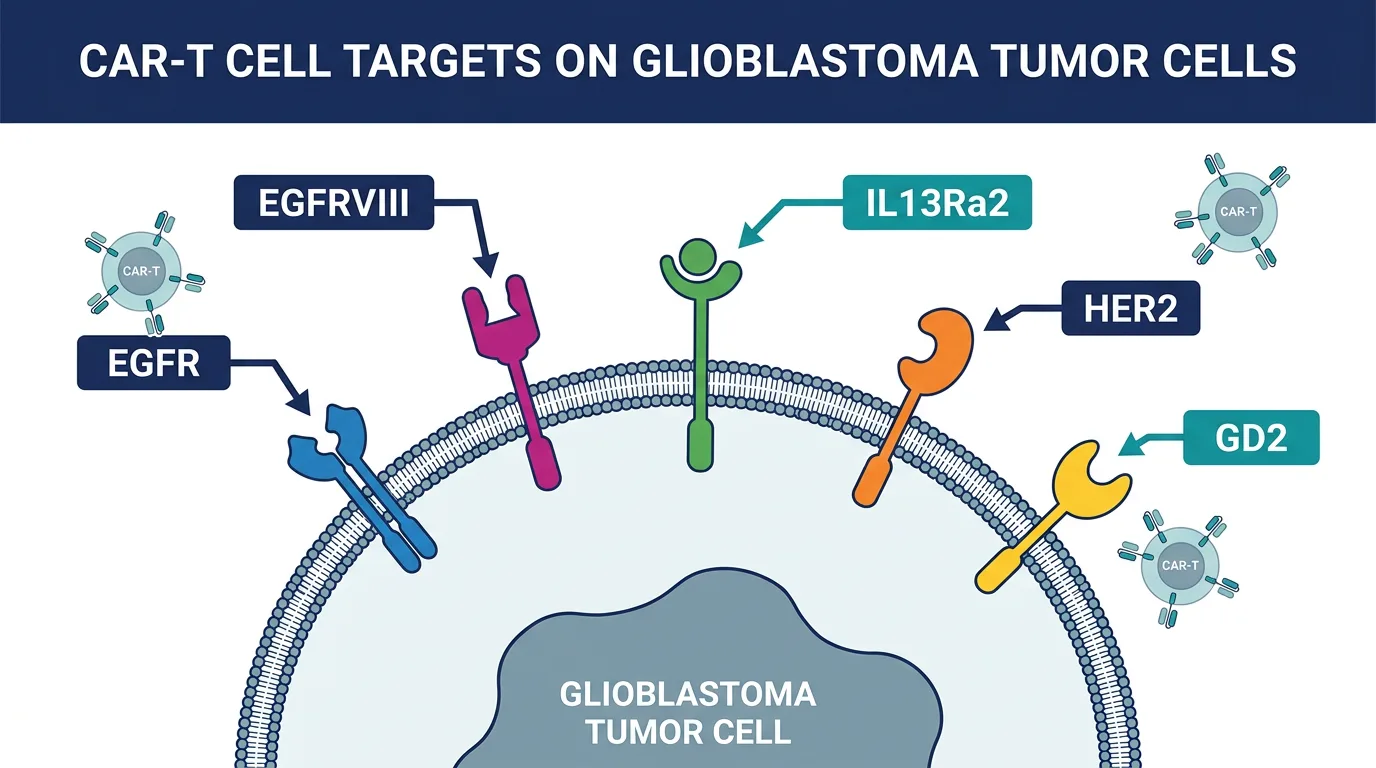
Understanding the Targets: What Your Tumor Needs to Express
CAR-T therapy only works if the CAR-T cells can find their target. Understanding these targets — and whether your tumor expresses them — is essential for evaluating trial eligibility.
| Target | Prevalence | Notes |
|---|---|---|
| EGFRvIII | 25–30% of GBMs | Found exclusively on cancer cells — ideal safety profile but limited patient population. |
| EGFR (Wild-Type) | 50–60% of GBMs | Not detected in normal brain tissue. Used by Penn and Mass General as a second target. |
| IL13Rα2 | 50–80% of GBMs | Rarely detectable in normal brain. Target of City of Hope's program and Penn's dual approach. |
| HER2 | ~42% of GBMs | Phase I safety demonstrated at Baylor. Less commonly pursued than EGFR/IL13Rα2. |
Questions to Ask Your Neuro-Oncologist
- Has my tumor been tested for EGFR amplification and/or EGFRvIII expression?
- What is my IL13Rα2 expression status?
- Can tissue from my surgery be sent for additional immunohistochemistry or FISH testing?
- If my tumor has recurred, has the target expression changed from my initial diagnosis?
An Honest Look at Limitations
Transparency: We believe patients deserve complete transparency about where CAR-T therapy stands today. The progress is real, but so are the limitations.
Responses Are Often Transient
Across the three major trials, dramatic initial tumor reductions have been observed — but in many cases, the tumors eventually regrow. The median duration of response is measured in weeks to months, not years.
Manufacturing Time and Complexity
CAR-T therapy is manufactured individually for each patient. The process typically takes 2–4 weeks — a meaningful delay for patients with rapidly progressing disease.
Eligibility Restrictions
Clinical trials have specific criteria. Many require adequate organ function, specific performance status scores, and particular molecular profiles. Discuss trial eligibility early — ideally at first recurrence.
Access and Geography
Current GBM CAR-T trials are concentrated at major academic centers: Penn Medicine (Philadelphia), Mass General (Boston), City of Hope (Duarte, CA). Access involves significant travel for many patients.
Safety Considerations
While intracranial delivery has been well tolerated overall, risks include neurological adverse events, cytokine release syndrome (usually manageable), and surgical risks from catheter placement. Across 128 patients treated in published trials, serious adverse events have primarily been neurological or hematological.
What Is Coming Next
The next generation of CAR-T approaches is designed to address durability and heterogeneity challenges head-on.
- Repeat Dosing Protocols — Both Penn and Mass General are studying multiple infusions over time. If one dose produces a temporary response, serial dosing may sustain immune pressure.
- Armored CAR-T Cells — CAR-T cells engineered to secrete pro-inflammatory cytokines (IL-12, IL-18) to remodel the immunosuppressive tumor microenvironment.
- Combination Strategies — CAR-T combined with checkpoint inhibitors, TTFields, LITT, and IL-15 agonists to enhance effectiveness.
- Moving to Newly Diagnosed Patients — Multiple programs plan to test CAR-T in newly diagnosed GBM — tumors may be more immunologically vulnerable before resistance evolves.
- AI-Driven Target Selection — AI is being used to identify optimal tumor-specific antigens, predict responses, and personalize CAR-T engineering.
How to Evaluate a CAR-T Trial
- Understand Your Molecular Profile — Ensure comprehensive profiling: IDH status, MGMT methylation, EGFR amplification/EGFRvIII status, and IL13Rα2 expression.
- Search ClinicalTrials.gov — Go to clinicaltrials.gov and search "CAR-T glioblastoma." Filter by location and recruitment status. Review eligibility criteria, target antigens, and delivery route.
- Contact Trial Sites Directly — Call the trial coordinator. Provide your molecular profiling results, treatment history, and functional status. Sites can often assess eligibility before you travel.
- Timing Matters — Discuss trial options early — ideally at initial diagnosis or first progression. Many trials exclude patients with extensive prior treatment.
- Get a Second Opinion — If your team isn't affiliated with a CAR-T trial site, seek a second opinion at a major academic center running these trials.
Currently Active CAR-T Trials in GBM (Early 2026)
| Trial | Target(s) | Phase | Setting | Key Site(s) |
|---|---|---|---|---|
| NCT05168423 | EGFR + IL13Rα2 (dual) | Phase I | Recurrent → Newly Diagnosed | Penn Medicine |
| NCT05660369 | EGFRvIII + EGFR (CAR-TEAM) | Phase I | Recurrent GBM | Mass General |
| NCT02208362 | IL13Rα2 | Phase I | Recurrent HGG | City of Hope |
| TGFβR2KO | IL13Rα2 (TGFβ-resistant) | Phase I | Recurrent/Progressive | Multiple sites |
| Emerging | GD2, B7-H3, HER2 | Phase I | Various | Various |
Trial availability and enrollment status change frequently. Always verify on clinicaltrials.gov.
The Bottom Line
CAR-T cell therapy for glioblastoma has moved from theoretical promise to demonstrated biological activity in patients. The 2025–2026 clinical data represents a genuine inflection point: for the first time, engineered immune cells are producing measurable tumor shrinkage in a cancer that has resisted every prior immunotherapy attempt.
But we must be honest. These are early-phase trials with small patient numbers. Responses are encouraging but often temporary. The field has not yet solved the durability problem.
What has changed is the trajectory. The question is no longer whether CAR-T cells can produce antitumor activity in GBM — they can. The question is now how to make those responses last.
For patients and families navigating GBM today, CAR-T therapy is not yet a standard treatment — it is an active frontier. Understanding that frontier, knowing your molecular profile, and engaging with trial opportunities early gives you the best chance of accessing what may become the next generation of GBM treatment.
Contact Information for Key Trial Sites
- Penn Medicine Abramson Cancer Center: 1-855-216-0098
- Mass General Cancer Center (INCIPIENT): 617-724-6226 | carteamingbm@mgb.org
- City of Hope: 626-218-2405
- ClinicalTrials.gov: Search "CAR-T glioblastoma"
References
- Bagley SJ, et al. Dual-target CAR T-cell therapy for recurrent glioblastoma. Nature Medicine, 2025. ASCO 2025 Abstract 102.
- Choi BD, et al. Rapid Regression of Recurrent Glioblastoma with CARv3-TEAM-E T Cells. NEJM, 2024. DOI: 10.1056/NEJMoa2314390.
- Brown CE, et al. Locoregional delivery of IL-13Rα2-targeting CAR-T cells in recurrent high-grade glioma. Nature Medicine, 2024.
- Begley SL, O'Rourke DM, Binder ZA. CAR T cell therapy for glioblastoma: A review of the first decade of clinical trials. Molecular Therapy, 2025; 33(6):2454-2461.
- iScience Review. CAR-T cell therapies for glioblastoma: early phase clinical trials and future perspectives. iScience, 2026; 29(2):114609.
- Systematic Review (2025). CAR-T-cell therapy for glioblastoma. Neuro-Oncology Advances, 2025; 7(1):vdaf115.
- npj Precision Oncology. CAR-T cell therapy for adult high-grade gliomas. 2024.
- Tang M, et al. Advancing glioblastoma immunotherapy. Pathology - Research and Practice, 2026; 278:156326.
- National Brain Tumor Society. New Brain Tumor Clinical Trials: November 2024 – June 2025.
This article is provided for educational purposes by the glioblastoma.center editorial team. It does not constitute medical advice. Treatment decisions should always be made in consultation with your neuro-oncology team. Clinical trial availability and eligibility criteria change frequently — always verify current information directly with trial sites.
Last reviewed: March 2026