The Most Important Molecular Test in Brain Tumor Oncology
When a neuro-oncologist hands you a pathology report, the first question is no longer just "what grade is it?" The question is: Does this tumor have an IDH mutation?
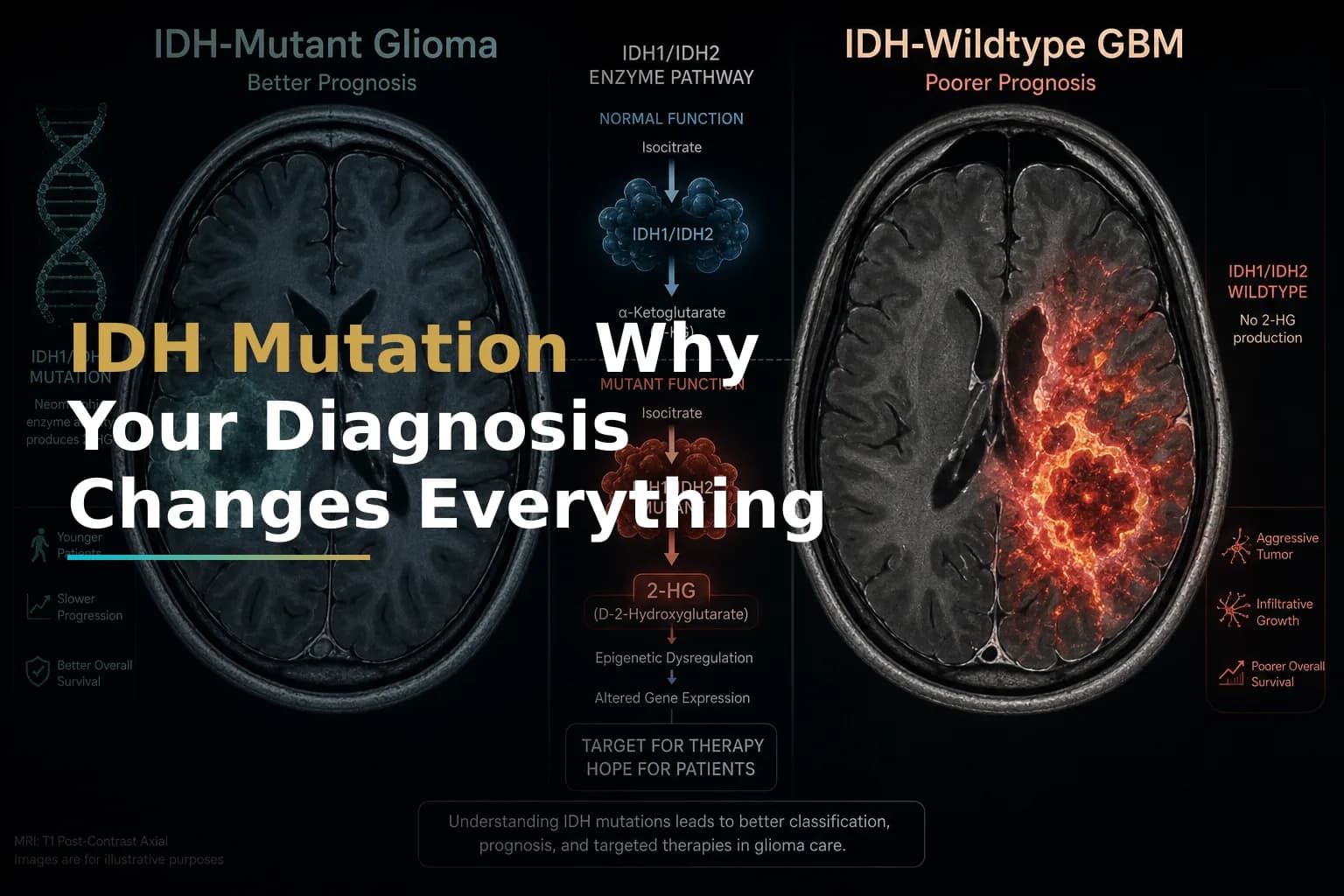
That single result — positive or negative — now separates two biologically distinct diseases. One is IDH-mutant glioma (most often astrocytoma or oligodendroglioma). The other is glioblastoma, IDH-wildtype. They can look similar on an MRI and even under a microscope. But at the molecular level, they behave differently, respond to different treatments, and carry very different outlooks.
This distinction determines which therapies are available, which clinical trials you may qualify for, and how aggressively your team should act. This article explains the science clearly so you can have sharper, more productive conversations with your care team.
What Is the IDH Gene — and What Does a Mutation Actually Mean?
IDH stands for isocitrate dehydrogenase, an enzyme involved in normal cell metabolism. In healthy cells, IDH converts isocitrate into alpha-ketoglutarate as part of the cell's energy cycle.
When the IDH1 or IDH2 gene mutates, the enzyme malfunctions. IDH enzymes contribute to cellular metabolism, and mutations to specific catalytic residues result in the neomorphic production of D-2-hydroxyglutarate (D-2-HG). The accumulation of D-2-HG results in epigenetic alterations, oncogenesis, and impacts the tumor microenvironment via immunological modulations.
In practical terms, this chemical buildup scrambles the cell's epigenetic "instruction manual," contributing to tumor formation. But here is the key paradox: mutations in the genes that make this enzyme lead to the production of a compound called D-2-hydroxyglutarate, which disrupts normal cell development and contributes to tumor growth. If tumor cells carry these mutations, they tend to respond better to treatment and be less aggressive than IDH wildtype tumors.
So the mutation causes the tumor — but it also makes the tumor more treatable. That tension is at the heart of why IDH status matters so much.
How the 2021 WHO Classification Redrew the Map
Until recently, the label "glioblastoma" was applied broadly to many high-grade brain tumors. That has changed.
In 2021, the WHO updated its classification system, bringing significant changes to how we diagnose and categorize glioblastoma. This classification system looks at specific alterations in the DNA of glioblastoma tumors to identify genetic mutations and alterations that drive glioblastoma growth and aggressiveness. The 2021 WHO classification system made two key changes to the criteria used to diagnose glioblastoma.
The most consequential change: as of 2021, the name glioblastoma is only given to tumors with unmutated, or "wildtype" IDH genes. By incorporating IDH wildtype status and other key genetic differences, the 2021 WHO classification system more accurately reflects the underlying molecular machinery that makes glioblastoma different from other cancer types. This can help doctors determine prognosis and assess treatment options.
The WHO Classification of CNS Tumors (2021) classifies adult-type diffuse glioma based on the presence of IDH mutations and other key molecular alterations as astrocytoma IDH mutant, oligodendroglioma IDH mutant and 1p/19q-co-deleted, and glioblastoma IDH-wildtype.
This is more than a naming convention. It reflects the fact that these are distinct tumor entities that originate from different pathological pathways and require tailored clinical management.
To understand your molecular profile more fully — including how IDH status relates to MGMT methylation and EGFR amplification — see our guide: Understanding Your GBM Molecular Profile: IDH, MGMT, EGFR & Why They Matter.
Who Gets Which Diagnosis?
IDH-mutant glioma is a type of brain tumor that happens when a gene called IDH changes in a way that affects how brain cells grow. Detecting an IDH mutation in the tumor cells from your biopsy or surgery leads to the diagnosis of IDH-mutant astrocytoma or oligodendroglioma. About 20% of gliomas have IDH mutations.
IDH-mutant gliomas tend to arise in younger adults, often presenting with seizures or other neurological symptoms in people in their 20s through 40s. Grade 2 gliomas, encompassing IDH-mutant astrocytomas and oligodendrogliomas, are characterized by distinct clinical, radiological, and molecular features. Clinically, they often present in younger adults (20–40 years) with seizures, focal neurological deficits, or incidental findings on imaging.
IDH-wildtype glioblastoma, by contrast, is the most common aggressive primary brain tumor in adults. The incidence of glioblastoma is 3.27 per 100,000 population and increases with age, peaking between 75 and 84 years. Median age at diagnosis is 66 years of age, making this often a disease of older individuals.
Additional molecular markers help sub-classify these tumors further:
- 1p/19q co-deletion: Defines oligodendroglioma (IDH-mutant). Associated with a particularly favorable chemotherapy response.
- CDKN2A/B homozygous deletion: Upgrades an IDH-mutant astrocytoma to WHO grade 4, even without the necrosis or vascular proliferation seen in classic GBM.
- EGFR amplification / TERT promoter mutation / +7/-10 chromosomal gain/loss: The system also classifies tumors that do not carry IDH mutations in the presence of other molecular features, such as EGFR amplification, TERT promoter mutation, or the gain of chromosome 7 with loss of chromosome 10 (+7/-10) to grade 4 glioblastomas regardless of their histologic appearance.
Prognosis: How Different Is the Outlook?
The prognosis gap between IDH-mutant glioma and IDH-wildtype glioblastoma is substantial and well-documented.
Median overall survival was 12.3 months for IDH-wildtype glioblastoma and 38.4 months for IDH-mutant astrocytoma in a large regional study of real-world outcomes. A single-center retrospective analysis published in PMC found a similar pattern, with median overall survival notably longer in the IDH-mutant group, at 16.0 months, versus 6.5 months in the wild-type group — reflecting a specific high-grade cohort where both groups were classified histologically as glioblastoma under prior criteria.
Across studies, patients with IDH-mutant astrocytomas generally have a more favorable prognosis than those with IDH-wildtype glioblastoma. And the discovery of mutations in the IDH1 and IDH2 genes in gliomas has significantly impacted the classification and treatment of these tumors. While histological grading has traditionally been used to predict prognosis in gliomas, it is now evident that IDH mutation status provides a more accurate indicator of a patient's clinical course.
However, this better prognosis comes with an important caveat. IDH-mutant gliomas tend to continually grow even after surgery and should be regularly checked with an MRI. They are not indolent. Recurrence is expected, and while IDH1 mutations significantly predicted longer time to first recurrence, they did not affect the interval between first and second recurrences. The mutation offers a real survival advantage early on, but vigilance remains essential at every stage.
Other factors also affect prognosis for IDH-wildtype GBM. The prognosis for patients with IDH-wildtype glioblastoma has remained poor despite major medical advances and extensive scientific efforts. Only a minority of patients experience survival beyond 5 years. Major favorable prognostic factors include younger age, gross total resection, and MGMT promoter methylation.
For more on how MGMT methylation shapes treatment decisions in glioblastoma, read: MGMT Methylation in Glioblastoma: What This Biomarker Really Means for Temozolomide Response and Your Treatment Plan.
Treatment: Where the Two Diagnoses Diverge
Both IDH-mutant glioma and IDH-wildtype glioblastoma share certain foundational treatment principles: maximum safe surgical resection, followed by radiation, then chemotherapy. But the details — and the emerging options — differ considerably.
IDH-Wildtype Glioblastoma: Standard of Care
For most patients with IDH-wildtype GBM, the backbone of treatment is the Stupp protocol: concurrent radiation with temozolomide chemotherapy, followed by adjuvant temozolomide. Tumor Treating Fields (TTFields) may be added for eligible patients. Because glioblastoma lacks a defined molecular target approachable by a small-molecule drug, treatment remains largely non-tumor-type-specific at this time, though MGMT methylation status guides decisions around chemotherapy and clinical trial eligibility.
For an in-depth look at one key component of recurrent GBM treatment, see: Bevacizumab for Recurrent Glioblastoma: What It Actually Does, Who It Helps, and What to Expect.
IDH-Mutant Glioma: A Targeted Therapy Era Has Arrived
The treatment landscape for IDH-mutant glioma shifted in 2024. On August 6, 2024, the FDA approved vorasidenib (Voranigo) to treat low-grade gliomas after surgery in adults and children aged 12 or older. Specifically, the approval covers the use of vorasidenib in people with grade 2 astrocytoma or oligodendroglioma with an IDH1 or IDH2 mutation.
Vorasidenib works by directly blocking the abnormal IDH enzyme. Vorasidenib citrate blocks the proteins made by the mutated IDH1 and IDH2 genes, which may help keep tumor cells from growing. It is a type of enzyme inhibitor and a type of targeted therapy.
This approval was based on the landmark INDIGO trial. Vorasidenib, a brain-penetrant dual inhibitor of mutant isocitrate dehydrogenase 1 and 2 (IDH1/2), represents a significant advancement in the management of IDH-mutant gliomas. This review explores the clinical implications of its recent FDA approval for grade 2 IDH-mutant astrocytomas and oligodendrogliomas. The pivotal INDIGO trial demonstrated substantial improvements in progression-free survival.
The National Brain Tumor Society called this a landmark moment: currently, for most grade 2 IDH-mutant diffuse glioma patients, the standard of care was a "watch and wait" approach, followed by chemotherapy and/or radiation when the tumor begins to grow more rapidly. Chemotherapy and radiation can be effective for these patients, but are not curative and have a number of negative side-effects. Delaying the need for these toxic treatments means patients can live longer without experiencing some of the long-term complications from these treatments.
This represents the first time a targeted treatment was successfully developed specifically for this patient population. And now that it has been shown that targeting IDH mutations in gliomas is an effective strategy, researchers and clinicians have the opportunity to explore more ways to leverage vorasidenib — as well as other potential IDH-targeting drugs — for additional glioma populations and in combinations with other treatments.
As reported by the National Cancer Institute, vorasidenib is the first targeted drug developed specifically for brain cancer to receive FDA approval — a milestone for the entire field.
Standard Treatment for IDH-Mutant Higher-Grade Glioma (Grades 3–4)
For IDH-mutant astrocytomas that are grade 3 or grade 4, treatment is more intensive. Standard of care therapy for IDH mutant gliomas starts with maximal safe resection when feasible. Surgery has both diagnostic and therapeutic objectives and, in the majority of the cases, is followed by a combination of radiation and chemotherapy. The specific chemotherapy regimen — temozolomide or the PCV combination of procarbazine, lomustine, and vincristine — depends on the tumor's histology, molecular markers, and grade.
Active Research and Clinical Trials
Research into IDH-targeted therapy is moving quickly beyond grade 2 tumors. The VIGOR trial (NCT06809322), launched in 2026, is evaluating vorasidenib as maintenance treatment after first-line chemoradiotherapy in IDH-mutant grade 2 or 3 astrocytoma in a placebo-controlled, randomized phase III study. This trial may further reshape the standard of care for higher-grade IDH-mutant disease.
A separate phase III study (NCT07215910) is investigating whether adding vorasidenib to the usual treatment, temozolomide, may be more effective than temozolomide alone in treating patients with newly diagnosed grade 3 astrocytoma after radiation therapy.
Beyond IDH inhibitors, researchers are studying immune-based strategies, combination regimens, and other molecular targets within IDH-mutant tumors. IDH mutation is a target for small molecule inhibition and immune therapy in diffuse astrocytomas and oligodendrogliomas.
To search for active trials, visit ClinicalTrials.gov and filter by "IDH mutant astrocytoma" or "IDH mutant glioma."
For a broader view of how the immunotherapy landscape is developing across glioma types, see: The Immunotherapy Landscape in GBM: Beyond Checkpoint Inhibitors.
What This Means for Newly Diagnosed Patients
If you have just received a brain tumor diagnosis, your most urgent step is to confirm that your tumor has been fully molecularly profiled. A complete pathology report in 2025 should include IDH1/2 mutation status, MGMT methylation status, 1p/19q co-deletion status, and other relevant markers. If this information is missing, ask your neuro-oncologist whether additional molecular testing is appropriate.
Knowing your IDH status changes the conversation in several concrete ways:
- Treatment eligibility: IDH-mutant grade 2 patients may now be eligible for vorasidenib, a targeted option not available to IDH-wildtype GBM patients.
- Clinical trial access: Many trials are IDH-stratified. Having the result documented opens or closes specific doors.
- Prognosis framing: IDH mutation status can help your team set a more accurate baseline expectation, which informs decisions about treatment intensity and surveillance frequency.
- Surveillance planning: Because even IDH-mutant tumors grow and recur, regular MRI follow-up remains essential regardless of tumor grade.
If you were recently diagnosed and are working through the first weeks of care, our article Newly Diagnosed Glioblastoma: What to Expect in the First 30 Days After Diagnosis provides a step-by-step orientation to the process.
When to Talk to Your Doctor
Contact your neuro-oncologist or care team if:
- Your pathology report does not include IDH mutation status, MGMT methylation status, or 1p/19q co-deletion results.
- You have an IDH-mutant grade 2 tumor and have not discussed whether vorasidenib or a clinical trial may be appropriate for your situation.
- You have been on a "watch and wait" protocol and have questions about when active treatment should begin.
- You experience new or worsening neurological symptoms between scheduled MRI appointments.
- You want to understand how your specific molecular profile affects your eligibility for emerging therapies or research studies.
This article is for general information and is not a substitute for medical advice. Always consult your oncologist or care team about your specific situation.