Why Your Pathology Report Mentions MGMT
After a glioblastoma diagnosis, your care team orders a molecular profile of your tumor. One of the first results they look at is MGMT methylation status. You may see the words "methylated" or "unmethylated" on your report. These terms carry real weight for how your oncologist plans chemotherapy and which clinical trials you may qualify for.
This article explains what the MGMT gene does, why its methylation state matters, what published evidence shows about treatment outcomes, and what your options look like depending on your result. For a broader look at all the molecular markers in your report, see our guide on Understanding Your GBM Molecular Profile: IDH, MGMT, EGFR & Why They Matter.
What Is MGMT and What Does It Do?
MGMT stands for O6-methylguanine-DNA methyltransferase. It is a gene that encodes a DNA repair enzyme. According to Mayo Clinic Laboratories, this enzyme repairs tumor cells from the DNA damage caused by alkylating chemotherapy agents. In plain terms: if the MGMT enzyme is active, it can undo the damage that drugs like temozolomide (TMZ) are trying to inflict on cancer cells.
Research published in Trends in Cancer (National Cancer Institute) explains the two-sided mechanism:
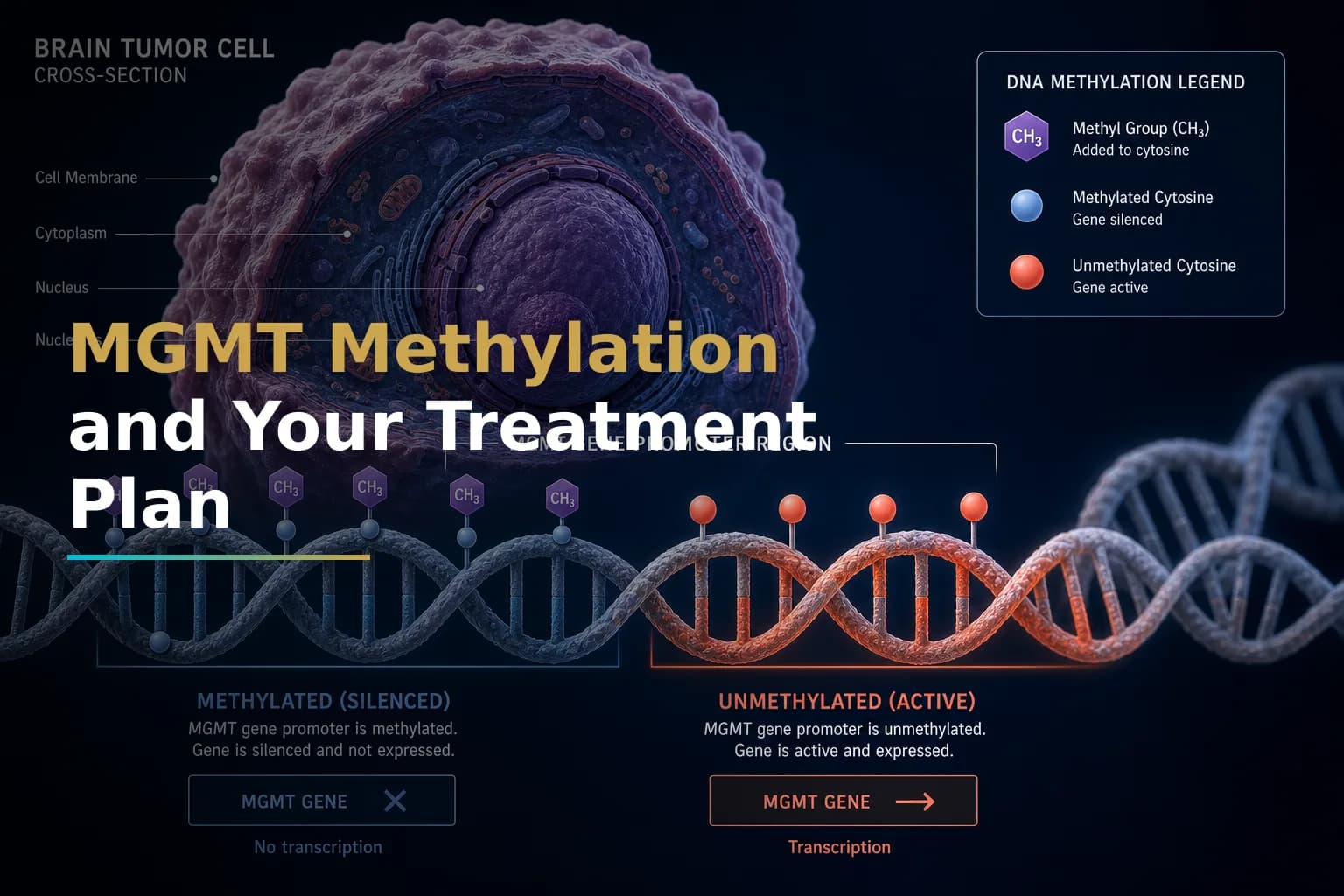
- When the MGMT promoter is methylated: The gene is silenced. The tumor produces little MGMT protein. This means the DNA damage from TMZ is not repaired, so the drug can do its job.
- When the MGMT promoter is unmethylated: The gene stays active. High levels of MGMT protein are expressed. The protein removes the alkylation damage that TMZ caused, promoting resistance to temozolomide.
Methylation silences the repair gene — and in this case, silencing that gene helps patients receiving TMZ.
How Common Is MGMT Methylation in Glioblastoma?
MGMT methylation is not rare. A large study in Cancers (2022) analyzed 321 consecutive IDH-wildtype glioblastoma patients and found a median overall survival of 12.6 months across the full group. Patients whose tumors showed at least 16% MGMT promoter methylation had meaningfully better survival than those with lower or no methylation. Roughly half of newly diagnosed glioblastoma patients carry some degree of MGMT methylation, though the exact percentage varies by testing method.
The degree of methylation also appears to matter, not just whether the result is positive or negative. The same study found that tumors with 1–15% methylation had survival similar to truly unmethylated tumors, suggesting a low methylation level may not provide the same benefit as a clearly methylated result.
The Evidence Behind MGMT as a Predictive Biomarker
The key data on MGMT comes from the EORTC 26981/22981 & NCIC CE.3 trial, which established concurrent temozolomide plus radiation as the standard of care. An analysis published alongside that trial found that patients with a methylated MGMT promoter had a median survival of 21.7 months and a 2-year survival rate of 46% when treated with temozolomide and radiotherapy — a clinically meaningful difference compared to unmethylated patients in the same trial.
Mayo Clinic Laboratories confirms that in newly diagnosed glioblastoma, MGMT promoter methylation is considered "an independent favorable prognostic biomarker and a strong predictor of response to alkylating chemotherapy."
MGMT methylation may also reflect a tumor that responds better to radiation. A study in Neuro-Oncology found that MGMT methylation predicted improved outcomes even among patients who received radiation alone, suggesting the biomarker may reflect broader tumor biology beyond chemo sensitivity. That said, methylation is a statistical signal, not a guarantee of response.
What MGMT Status Means for Your Treatment Decisions
Standard of care for glioblastoma is surgical resection followed by radiotherapy and temozolomide chemotherapy. MGMT status does not change that protocol for most patients, but it does influence several decisions:
For Older or Frailer Patients
Full concurrent chemoradiation is demanding. Research published in Advances in Therapy notes that combined chemoradiotherapy may be too toxic for elderly patients. For this group, MGMT status helps decide between TMZ alone versus radiation alone. In methylated patients, TMZ tends to be more effective. In unmethylated patients, radiation alone may be the better-tolerated and more effective choice. Mayo Clinic Laboratories specifically notes that for patients over 60–65 years, MGMT status guides this decision.
For Newly Diagnosed, Fit Patients
Your team will likely recommend the Stupp protocol (concurrent TMZ plus radiation, then adjuvant TMZ) regardless of MGMT status. But your result informs how closely your response is tracked and how actively your team may seek clinical trials. A methylated result means you are considered more likely to benefit from TMZ. An unmethylated result may prompt your team to discuss trials exploring alternative or additional agents.
At Recurrence
MGMT status is generally stable throughout the disease course. Analyses of paired primary and recurrent tumor samples have found that MGMT promoter methylation status is typically unchanged from first diagnosis to recurrence, so the result from your original biopsy may still be relevant when making decisions at recurrence. For more on this topic, see our guide on Recurrent GBM: Why It Comes Back, What You Can Do, and How to Navigate What Comes Next.
The Challenge of the Unmethylated Result
An unmethylated MGMT result is genuinely more difficult. It is not a reason to abandon treatment, but it does mean that standard TMZ may be less effective, and your team may need a more active strategy.
A reanalysis of three phase III trials published in Neuro-Oncology (2024) confirmed that glioblastoma with truly unmethylated MGMT promoter showed no statistically meaningful benefit from temozolomide in elderly patients. The authors concluded that validated MGMT methylation assays should be used to identify truly unmethylated patients so they can be directed toward more promising options without the added toxicity of a drug unlikely to help them.
An ASCO clinical commentary states that for patients with truly unmethylated MGMT, enrollment in clinical trials should be a priority. Several trials are actively exploring alternative and combination approaches for this population. Completed trials such as CheckMate-498 (NCT02617589) examined nivolumab plus radiation as an alternative to TMZ in unmethylated GBM, and results from those efforts continue to shape available options.
If your tumor is unmethylated, you may want to discuss:
- Clinical trial enrollment as a first-line option
- Whether tumor treating fields (TTFields) add value in your case
- Targeted therapy options based on other molecular markers in your profile (EGFR, TERT, etc.)
- Newer approaches being studied for this population, such as PI3K/AKT/mTOR pathway inhibitors — see our article on Paxalisib and the MGMT Unmethylated Problem: Finally, an Option?
How Is MGMT Status Tested?
MGMT methylation is measured from tumor tissue removed during surgery or biopsy. Several laboratory techniques are used:
- Methylation-specific PCR (MSP): The most widely used method in clinical practice. It gives a binary methylated/unmethylated result.
- Pyrosequencing: A more quantitative approach that measures the percentage of methylation at specific CpG sites in the MGMT promoter. Research in Clinical Neuropathology established that pyrosequencing meets high analytical performance standards and can be recommended for routine clinical use when strict quality controls are applied.
- Next-generation sequencing (NGS): Used in comprehensive molecular panels and increasingly available at major cancer centers.
The testing method matters. Results can differ between platforms, and the cutoff for calling a tumor "methylated" varies by lab. If you have a borderline result — such as a low methylation percentage by pyrosequencing — ask your oncologist whether the quantitative value, not just the binary call, is being factored into your plan.
A review in Neuro-Oncology notes that despite the importance of this biomarker, routine clinical use has faced real challenges, including lab-to-lab variability, lack of standardized cutoffs, and no validated alternative for unmethylated patients. Knowing this helps you ask better questions at your next appointment.
Where MGMT Fits in the Broader Molecular Picture
MGMT methylation does not act in isolation. Your tumor's biology is shaped by a collection of molecular changes. IDH mutation status, EGFR amplification, TERT promoter mutations, and CDKN2A deletion all interact with MGMT to influence prognosis and treatment response. NCI-supported research points out that gaps between MGMT promoter methylation status and actual treatment response exist in some patients — likely because MGMT protein expression is not always perfectly predicted by promoter methylation alone.
This is one reason your oncologist considers the full molecular profile rather than a single result. If you are still building your understanding of that broader picture, see our article on Newly Diagnosed Glioblastoma: What to Expect in the First 30 Days After Diagnosis.
Some researchers are also examining whether MGMT status interacts with metabolic approaches. The ketogenic diet, for example, may theoretically complement the DNA-damage mechanisms of TMZ, though this remains early-stage investigation. Our article on the Ketogenic Diet and Glioblastoma: What the Evidence Actually Says covers this in detail. Some drug repurposing strategies — including valproic acid, which has HDAC-inhibiting properties — are also being studied in the context of MGMT regulation and epigenetic silencing. See Valproic Acid and Glioblastoma: Can an Anti-Seizure Medication Also Help Fight Your Tumor? for more.
The Limits of What MGMT Status Can Tell You
It is worth being clear about what this biomarker does and does not predict:
- MGMT methylation is a probabilistic predictor — it shifts the odds, but does not determine your individual outcome.
- Some methylated patients do not respond well to TMZ; some unmethylated patients have unexpectedly durable responses.
- MGMT status is one input into a complex decision, not a verdict.
- As Neuro-Oncology experts note, "the clinical management of patients based on the MGMT promoter methylation status should be considered together with other molecular and clinical factors that contribute to patient outcome."
Use this result as a tool for an informed conversation, not as a ceiling on your expectations.
When to Talk to Your Doctor
Talk to your neuro-oncologist if you have not yet received your MGMT methylation result, if your result was borderline or showed a low quantitative methylation percentage, if you want to understand how your result is shaping your current treatment plan, or if you are interested in clinical trials designed for your specific MGMT status. Ask directly: "What testing method was used, and what was the quantitative methylation level?" That detail may be clinically relevant, especially if your result falls near the threshold between positive and negative.
This article is for general information and is not a substitute for medical advice. Always consult your oncologist or care team about your specific situation.