Key Takeaways
- Recurrence in glioblastoma is near-universal. It is not a failure of treatment or a failure of the patient — it is a fundamental feature of this disease's biology.
- 80–90% of recurrences develop within 2 cm of the original tumor site, arising from infiltrative cancer cells that surgery and radiation cannot fully eliminate.
- Glioma stem cells — a therapy-resistant subpopulation that can self-renew, hide in protective niches, and regenerate the tumor — are the primary engine driving recurrence.
- There is no established standard of care for recurrent GBM. Treatment decisions are individualized and require honest conversations about goals, options, and quality of life.
- Emerging approaches — including CAR-T cell therapy, re-irradiation with bevacizumab, immunotherapy combinations, and adaptive platform trials — represent genuine progress, but access requires early planning.
- Quality of life at recurrence is not a secondary concern — it is the central concern.
The Hardest Conversation in Neuro-Oncology
If you are reading this article, you or someone you love has likely heard the words that every GBM patient dreads: the tumor is growing again.
Recurrence is the defining feature of glioblastoma. Despite surgery that removes every visible trace of tumor, despite six weeks of daily radiation, despite months of temozolomide chemotherapy — in nearly every case, the disease comes back. This is not because the treatment failed. It is because glioblastoma, at a fundamental biological level, is designed to survive what we throw at it.
Understanding why recurrence happens is not an academic exercise. It is the key to making informed decisions about what to do next, which clinical trials might be worth pursuing, and how to balance the pursuit of disease control against the preservation of the life you want to live.
Why Glioblastoma Comes Back: The Biology of Recurrence
Recurrence is not random. It is driven by specific, well-characterized biological mechanisms that the tumor has evolved to exploit.
1. The Infiltration Problem
When a neurosurgeon removes a glioblastoma, they remove everything they can see. But glioblastoma is not a contained ball of cancer. Individual tumor cells migrate along white matter tracts, blood vessels, and the spaces between neurons, spreading far beyond the visible boundary.
This is why 80–90% of GBM recurrences develop within 2 cm of the original tumor site. The cells that seed the recurrence were already there — embedded in apparently normal brain tissue — before the first surgery was ever performed.
2. Glioma Stem Cells: The Root of Regrowth
Perhaps the most important discovery in GBM biology over the past two decades is the identification of glioma stem cells (GSCs) — a small subpopulation with extraordinary capabilities:
- Self-renewal: A single GSC can divide to produce both another stem cell and a differentiated tumor cell, ensuring the pool is never depleted.
- Multipotency: They can regenerate the full spectrum of cell types in the tumor.
- Treatment resistance: Enhanced DNA repair, drug efflux pumps, and metabolic adaptations let them survive radiation and temozolomide.
GSCs also exploit hypoxic niches where low oxygen activates survival pathways (HIF-1α) that keep them dormant — alive but not dividing. Because most treatments target dividing cells, quiescent GSCs are effectively invisible.
Even if treatment eliminates 99.9% of tumor cells, the surviving GSCs are sufficient to regrow the entire tumor.
3. Molecular Evolution Under Treatment Pressure
Treatment itself reshapes the tumor. A critical example is temozolomide-induced hypermutation: some GBMs acquire mutations in DNA mismatch repair genes (MSH6, MSH2, MLH1), accumulating extreme numbers of new mutations that drive resistance.
EGFR expression frequently shifts between primary and recurrent tumors. Research on matched samples shows the molecular makeup differs in every pair — the recurrent tumor is, in many respects, a different disease from the one originally treated.
4. The Immunosuppressive Fortress
The microenvironment around a recurrent GBM is profoundly immunosuppressive — more so than the primary tumor. Recurrent tumors recruit regulatory T cells, myeloid-derived suppressor cells, and tumor-associated macrophages that actively suppress immune responses.
This is a major reason why single-agent checkpoint inhibitors have shown limited efficacy in recurrent GBM, despite transformative success in other cancers.
5. Therapy-Induced Cellular Plasticity
A 2025 study documented recurrent GBM cells acquiring a radial glia-like phenotype — a cell type normally seen during brain development — that was entirely absent in the primary tumor. These transformed cells exhibited rapid adhesion and elongated processes that facilitated cancer cell migration.
Treatment does not just kill vulnerable cells. It applies selective pressure that drives survivors toward more aggressive, more adaptable phenotypes.
Treatment Options at Recurrence
There is no established standard of care for recurrent GBM. Unlike primary treatment (Stupp protocol), recurrence requires individualized decision-making between you, your neuro-oncologist, and your neurosurgeon.
Re-Resection (Second Surgery) — Case-by-case
Repeat surgery may be considered if the tumor is accessible and a meaningful extent of resection is achievable. Median survival after re-resection: 6–17 months. Re-resection also provides fresh tissue for updated molecular profiling — invaluable for trial eligibility.
Bevacizumab (Avastin) — Symptom relief
Reduces brain swelling, often dramatically improves symptoms (headaches, neurological deficits), and extends progression-free survival (~4 months). PFS-6 rates: 29–43%.
However: The phase 3 EORTC 26101 trial found no significant overall survival difference (9.1 vs. 8.6 months). Bevacizumab is a symptomatic treatment that improves quality of life but does not durably control the disease.
Lomustine (CCNU) — Baseline standard
The most commonly used chemotherapy control arm in recurrent GBM trials. Objective response rate: ~10%. Median PFS: <2 months. PFS-6: ~20%. Median OS: 7–8.6 months. These numbers are sobering, but represent an honest baseline.
Temozolomide Rechallenge — MGMT-dependent
Evidence is limited. For MGMT methylated patients, rechallenge may provide modest benefit. For unmethylated patients, the biological rationale is weak.
Re-Irradiation — Growing evidence
Median OS: 7–13 months. Meta-analyses suggest improved outcomes when combined with bevacizumab or lomustine. The phase III LEGATO trial (EORTC-2227-BTG) will provide definitive data.
Tumor Treating Fields (TTFields) — Under investigation
Typically used in the newly diagnosed setting, TTFields are being evaluated at recurrence in combination with novel agents. Some patients continue TTFields through recurrence.
The Clinical Trial Imperative
For patients with recurrent GBM, clinical trials are not a last resort — they are often the best available option. But accessing them requires planning, timing, and honest conversations.
The Single Most Important Advice: Discuss clinical trial options early — at first suspicion of progression, not after exhausting standard options. Every treatment you receive before entering a trial can potentially close doors. Having the trial conversation early preserves the maximum number of options.
Key Trials to Know About
- CAR-T Cell Therapy — Penn Medicine's dual-target CAR-T (EGFR + IL13Rα2), Mass General's CAR-TEAM (EGFRvIII + EGFR), and City of Hope's IL13Rα2 program have all shown tumor shrinkage in recurrent patients. Read more
- Anktiva + NK cells + TTFields — A chemotherapy-free immune activation combination that achieved 100% disease control in a 5-patient pilot study — now recruiting for phase 2.
- LEGATO Trial (EORTC-2227-BTG) — Phase III randomized trial of re-irradiation + lomustine vs. lomustine alone — the first definitive trial on re-irradiation.
- GBM AGILE — Adaptive platform trial evaluating multiple therapies simultaneously in both newly diagnosed and recurrent patients using biomarker stratification.
- Neoadjuvant Pembrolizumab — Administered before surgery at recurrence — showed unexpected survival benefit in phase II. Phase IV confirmatory study (NCT05235737) now underway.
How to Navigate Trial Access
- Search clinicaltrials.gov for "recurrent glioblastoma" — filter by "Recruiting" status and your location.
- Contact trial sites directly — phone calls to coordinators often yield more than online portals.
- Consider a second opinion at a major neuro-oncology center (Dana-Farber, UCSF, MD Anderson, Memorial Sloan Kettering, Penn Medicine, Mass General).
Pseudoprogression: When "Growth" Is Not Growth
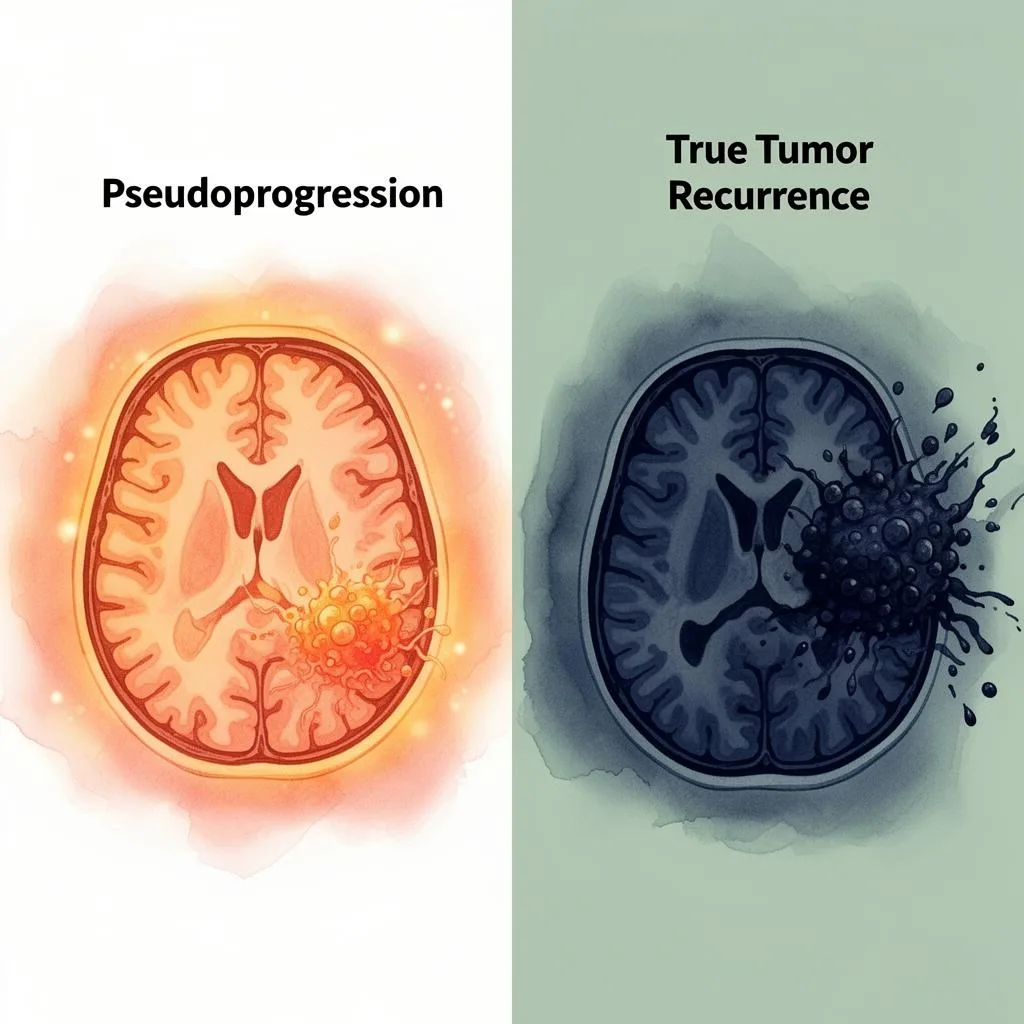
Pseudoprogression occurs in approximately 20–30% of GBM patients, and is more common in MGMT methylated tumors. It typically occurs within the first 3–6 months after completing initial treatment.
Distinguishing pseudoprogression from true recurrence is one of the most challenging problems in neuro-oncology. Advanced imaging — including perfusion MRI, MR spectroscopy, and amino acid PET — can help, but none is definitive.
What to Ask Your Doctor: If your MRI shows growth early after treatment, ask specifically about pseudoprogression. If there is genuine uncertainty, a period of watchful waiting with serial imaging may be more appropriate than immediately changing treatment.
Living With Recurrent GBM: The Quality of Life Reality
Treatment decisions at recurrence must be made in the full context of how you are living, not just how long you might live.
Fatigue
Up to 90% of patients with tumor recurrence experience fatigue — a profound, unpredictable exhaustion that limits daily life. It doesn't reliably improve with rest.
Management: structured activity pacing, corticosteroid optimization, screening for treatable factors (anemia, thyroid, depression).
Seizures & Anti-Epileptics
Seizures can increase at recurrence. Levetiracetam (Keppra) is effective but can cause significant behavioral side effects — "Keppra rage."
If experiencing personality changes or irritability, ask about alternatives: lacosamide, brivaracetam, valproic acid. Never stop Keppra abruptly.
Cognitive Decline
Memory difficulties, word-finding problems, slowed processing, and loss of executive function are common — caused by the tumor, treatment, medications, or all three.
Cognitive rehabilitation therapy and simple accommodations (written reminders, simplified routines) can meaningfully preserve independence.
Caregiver Burden
Caregivers report high rates of anxiety, depression, sleep disruption, and burnout. The emotional labor of managing medications, coordinating care, and witnessing changes is immense.
CancerCare Hopeline: 800-813-4673 (free counseling). If you are a caregiver, take your own wellbeing seriously.
Palliative Care Is Not Giving Up
Palliative care is not hospice. It is specialized medical care focused on relieving symptoms, managing pain, and improving quality of life — and it can run in parallel with active, aggressive treatment from diagnosis onward.
Studies across multiple cancer types show early palliative care integration improves both quality of life and, in some cases, overall survival. If palliative care has not been discussed, ask for it.
Planning Ahead: Conversations That Matter
Advance Directives & Goals of Care
If you have not completed an advance directive or healthcare power of attorney, recurrence is the time. These documents ensure your wishes are honored. This is not pessimism — it is respect for your own autonomy.
Honest Prognosis Conversations
You have the right to ask for an honest assessment — and the right not to ask. If you do want to know, frame it specifically: "Based on my molecular profile, my performance status, and the available data, what is a realistic range of outcomes?"
What Matters Most to You
The question driving every treatment decision should not be "which treatment adds the most days?" but rather "what does a good day look like for me, and which strategy is most likely to preserve that?" There is no wrong answer — only your answer.
Research References
- Glioma Stem Cells in tumor heterogeneity, immune evasion, and therapeutic resistance. Cancers, 2025; 17(8). — PMC
- Hunting glioblastoma recurrence: glioma stem cells as retrospective targets. Am J Physiol — Cell Physiol, 2025. — APS Journals
- GBM: An overview of current therapies and mechanisms of resistance. Pharmacological Research, 2021. — PMC
- Singh S, et al. Glioblastoma at the crossroads. Signal Transduction and Targeted Therapy, 2025; 10:213. — Nature
- Recurrent Glioblastoma: From Molecular Landscape to New Treatment Perspectives. Cancers, 2021; 13(3):464. — PMC
- Recurrent Glioblastoma: A Review of the Treatment Options. Cancers, 2023; 15(17):4279. — PMC
- Wick W, et al. Lomustine and Bevacizumab in Progressive Glioblastoma. NEJM, 2017; 377:1954–1963. — NEJM
- Treatment options for progression or recurrence of glioblastoma: a network meta-analysis. Cochrane, 2021. — PMC
- ESTRO/EANO recommendation on reirradiation of glioblastoma. Radiotherapy and Oncology, 2025; 204:110696. — LWW
- Molecular markers in GBM prognosis and recurrence patterns. Cancer Biology & Therapy, 2025. — Taylor & Francis
- Atypical behavior of recurrent GBM tumor cells with a radial glial phenotype. Cogent Biology, 2025. — Taylor & Francis
- Unlocking glioblastoma: breakthroughs in molecular mechanisms. Molecular Biology Reports, 2025. — PMC
- National Brain Tumor Society. Let's Talk About Glioblastoma. 2025. — NBTS
- Treating recurrent glioblastoma: an update. Cancer Medicine, 2018. — PMC
- Bevacizumab combined with re-irradiation in recurrent glioblastoma. Frontiers in Oncology, 2022. — PMC
Resource Directory for Patients and Caregivers
| Resource | Contact | What They Offer |
|---|---|---|
| CancerCare Hopeline | 800-813-4673 / cancercare.org | Free counseling, financial assistance, support groups |
| National Brain Tumor Society | braintumor.org | Patient navigation, clinical trial matching, advocacy |
| American Brain Tumor Association | 800-886-ABTA / abta.org | Education, support, treatment center directory |
| ClinicalTrials.gov | clinicaltrials.gov | Searchable database of all registered clinical trials |
| NBTS Patient Navigator | braintumor.org/support | One-on-one guidance for treatment decisions |
This article is provided for educational purposes by the glioblastoma.center editorial team. It does not constitute medical advice. Treatment decisions should always be made in consultation with your neuro-oncology team. If you or a loved one is experiencing a mental health crisis, please contact the 988 Suicide and Crisis Lifeline by calling or texting 988.
Last reviewed: March 2026