Why Researchers Are Looking at Cholesterol-Lowering Drugs for Brain Tumors
Statins are best known for keeping hearts healthy. Millions of people take them every day to lower their cholesterol and reduce their risk of heart attack or stroke. But for more than two decades, scientists have been asking a different question: can a drug that blocks cholesterol production also block the growth of one of the most aggressive brain tumors known?
Glioblastoma (GBM) is a high-grade glioma that is extraordinarily difficult to treat. Despite surgery, radiation, and temozolomide chemotherapy, median survival is roughly 12 to 18 months after diagnosis. That harsh reality has pushed researchers and integrative oncologists to look at drugs already in wide use — drugs with known safety profiles, low cost, and the ability to cross into the brain — as possible additions to standard care. Statins fit that description well.
This article explains what statins are, why GBM cells appear vulnerable to them at the molecular level, what current evidence says about their role alongside standard treatment, and what remains unresolved.
What Are Statins and How Do They Work?
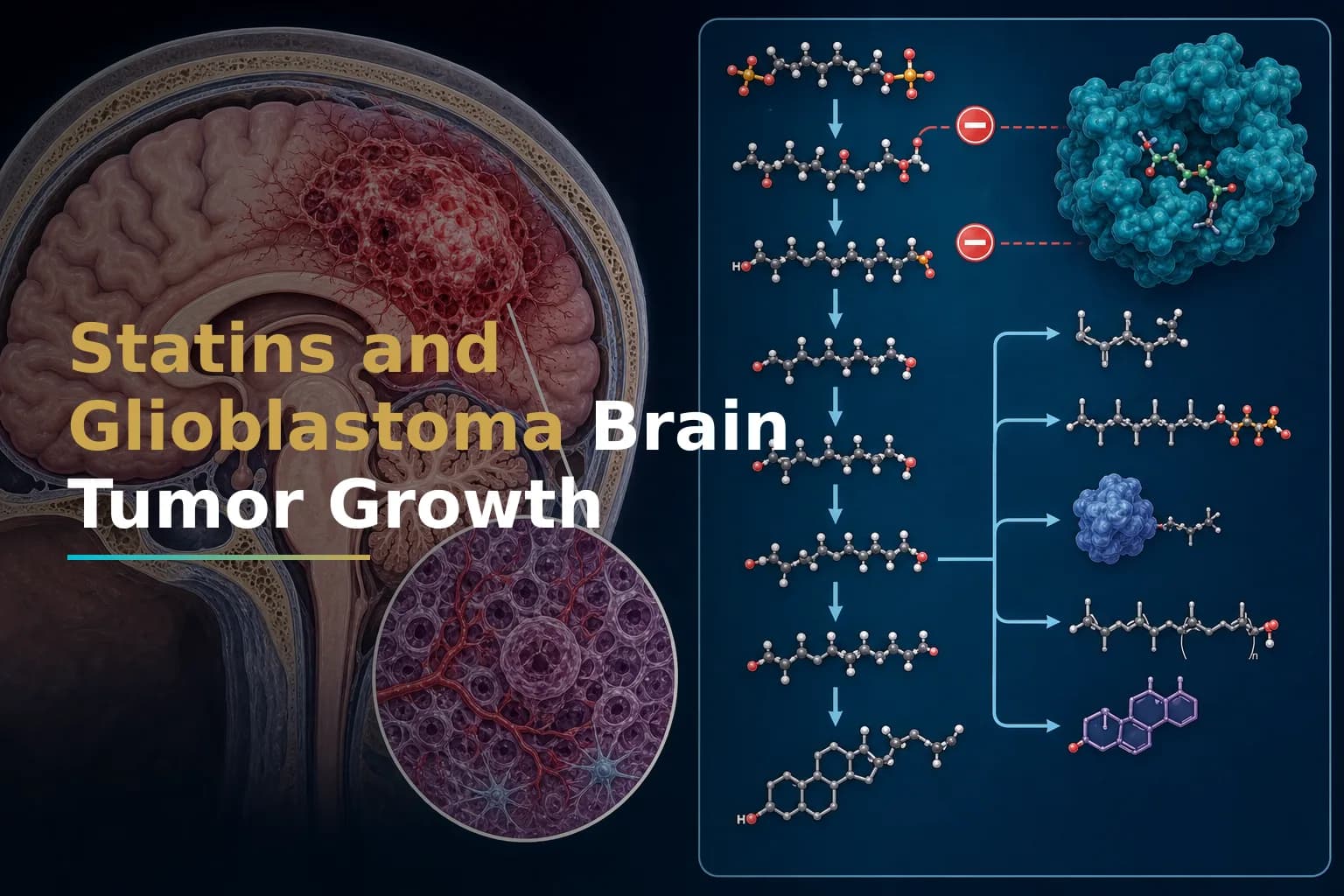
Statins are competitive inhibitors of HMG-CoA reductase (HMGCR) — the enzyme that controls the rate-limiting step in the mevalonate pathway, which is the biochemical route through which the body makes cholesterol. By blocking this enzyme, statins lower circulating cholesterol and reduce cardiovascular risk.
Beyond lowering lipids, statins have what researchers call "pleiotropic" effects — biological actions unrelated to cholesterol. These include reducing inflammation, changing cell signaling, and interfering with molecules that tumor cells depend on for growth and survival.
The statins most studied in GBM include simvastatin, lovastatin, atorvastatin, fluvastatin, and pitavastatin. All are FDA-approved and widely available. Importantly, some are lipophilic (fat-soluble), which means they cross the blood-brain barrier more readily than hydrophilic statins such as pravastatin or rosuvastatin.
Why Glioblastoma Cells Depend Heavily on Cholesterol
The brain has the highest cholesterol concentration of any organ, and GBM cells exploit that environment aggressively. GBM cells are metabolically dependent on exogenous cholesterol uptake, making them vulnerable to agents that target their cholesterol intake or alter cholesterol efflux.
GBM cells accumulate cholesterol in structures called lipid rafts — specialized regions of the cell membrane that act as signaling platforms and drug-entry channels. Research has shown that SOAT1, an enzyme critical for cholesterol esterification, is overexpressed in GBM cells, and this overexpression promotes lipid accumulation and tumor development. Disrupting this metabolic dependency is a key target for statin researchers.
Elevated LDL cholesterol has also been linked to resistance to temozolomide, the standard GBM chemotherapy drug. Research suggests that increased cholesterol levels may promote resistance to chemotherapy by upregulating drug-efflux proteins such as ABCG1 and MDR1. If statins can reduce cholesterol availability in tumor cells, they may help restore sensitivity to standard drugs.
To learn more about how your tumor's molecular profile shapes treatment response, see our guide: Understanding Your GBM Molecular Profile: IDH, MGMT, EGFR & Why They Matter.
The Mevalonate Pathway: The Central Target
The mevalonate pathway does more than make cholesterol. It also produces intermediate molecules — farnesyl pyrophosphate (FPP) and geranylgeranyl pyrophosphate (GGPP) — that attach to proteins called Rho-GTPases and Ras-family GTPases. These proteins control how tumor cells grow, migrate, invade surrounding tissue, and resist treatment.
A 2023 study published in Neuro-Oncology added another layer to this picture. Researchers found that when GBM cells survive radiation treatment, they activate the mevalonate pathway as part of a recovery response. Combination treatments that activate the mevalonate pathway in GBM cells after sublethal treatment enhance self-renewal and migratory capacity through Rac-1 activation — a metabolic vulnerability that may potentially be exploited using statins. In other words, treating GBM with radiation may make tumor cells more dependent on the mevalonate pathway, which statins could then disrupt.
This connects directly to the challenge of recurrence, a topic explored further in our article on Recurrent GBM: Why It Comes Back, What You Can Do, and How to Navigate What Comes Next.
Preclinical Evidence: What Lab and Animal Studies Show
The preclinical case for statins in GBM is compelling. In laboratory screens of FDA-approved drugs, statins consistently showed meaningful anti-GBM activity. A screen of 446 FDA-approved drugs found that statins were active in vitro, inhibiting GBM cell proliferation and inducing cellular autophagy, and they enhanced the pro-apoptotic activity of another cancer drug by 40 to 70 fold.
Simvastatin and lovastatin have both been studied in combination with temozolomide (TMZ). Laboratory results showed that lovastatin may enhance the cytotoxicity of temozolomide, increase TMZ-induced cellular apoptosis, and impair autophagic flux in GBM cells — a mechanism associated with enhanced cell death. A separate research group found that simvastatin combined with TMZ decreased GBM cell viability and significantly increased apoptotic cell death compared to either drug alone.
Beyond direct cell killing, statins have been shown to inhibit tumor angiogenesis (the formation of new blood vessels that feed tumors), reduce inflammation within the tumor microenvironment, and interfere with the TGF-β signaling pathway, which allows GBM to suppress immune responses and promote invasion.
Researchers have also noted that lipid rafts — cholesterol-rich membrane domains that GBM cells use for invasion and drug resistance — are disrupted when cholesterol metabolism is altered. Cholesterol helps maintain the integrity of lipid rafts, and disrupting cholesterol metabolism may impair the lipid raft microstructure that cancer cells rely on in multiple ways.
Preclinical research suggests statins work through several parallel mechanisms rather than a single pathway. That breadth of action is part of what makes them interesting as potential adjuncts, but it also makes it harder to predict who will benefit most.
Clinical Evidence: Promising but Not Yet Conclusive
Moving from the lab to the clinic is where things get more complicated. The honest summary of the clinical data is: suggestive, but not yet definitive.
One large cohort study from the Danish Cancer Registry, which identified more than 1,500 patients diagnosed with GBM, found that statin use before diagnosis was associated with a trend toward improved overall survival. A separate meta-analysis also noted that pre-diagnosis statin use favored overall survival, with a hazard ratio of 0.85 in a subgroup analysis — suggesting roughly a 15% relative reduction in mortality risk among pre-diagnosis users. However, the effects of statins on survival in patients with glioblastoma remain controversial, and preclinical antitumor activity has not yet translated into clear clinical benefit in prospective trials.
A study of 1,093 patients with high-grade glioma from a regional cancer registry found that statins and NSAIDs inhibit glioma cell growth in vitro and in vivo, but data on statin treatment in relation to survival of patients with high-grade glioma from clinical studies remain sparse and inconclusive.
There are several reasons clinical results have been harder to interpret than lab data:
- Heterogeneity of statin types. Lipophilic statins (simvastatin, lovastatin) penetrate the blood-brain barrier more readily than hydrophilic statins, but many studies group all statins together.
- Timing and duration. Most observational studies capture patients already taking statins for cardiac reasons. Whether starting statins at GBM diagnosis produces different results is still under study.
- Confounding factors. Patients prescribed statins tend to have different overall health profiles than those who are not, making it hard to isolate the statin effect in observational data.
- Dose and molecular subtype. Laboratory studies often use doses that may not be safely achievable in the brain. GBM's molecular subtypes (IDH-wildtype vs. IDH-mutant, MGMT-methylated vs. unmethylated) may also influence statin sensitivity in ways observational data cannot capture.
For context on how molecular markers shape GBM treatment strategy, see: MGMT Methylation in Glioblastoma: What This Biomarker Really Means for Temozolomide Response and Your Treatment Plan.
Statins in the Broader Drug-Repurposing Landscape
Statins are one of several already-approved medications being studied as possible adjuncts for GBM. Drug repurposing — using existing drugs for new purposes — is attractive because these compounds have already cleared regulatory safety hurdles and cost far less than novel targeted therapies.
Drug repurposing has become of increasing interest in high-grade glioma research, with statins among the key candidates under investigation alongside other metabolic agents. Their appeal grows further because many statins are inexpensive generics already stocked in hospital formularies worldwide.
Statins are being studied alongside other repurposed candidates such as metformin and valproic acid. For how those agents compare, see: Metformin and Glioblastoma: Can a Common Diabetes Drug Help Fight Your Brain Tumor? and Valproic Acid and Glioblastoma: Can an Anti-Seizure Medication Also Help Fight Your Tumor?
No repurposed drug has yet shown clear survival benefit in a prospective phase III GBM trial. Still, the mechanistic rationale for statins — particularly their ability to disrupt a pathway that GBM cells rely on after treatment — continues to drive scientific interest and supports ongoing clinical investigation.
Key Concerns and Limitations to Know
Any discussion of statins and GBM must also address real limitations and risks.
- Known side effects. Statins are generally well tolerated but can cause muscle pain (myopathy), liver enzyme elevations, and a small increase in type 2 diabetes risk in some patients. These effects must be monitored.
- Blood-brain barrier penetration. Not all statins reach useful concentrations in the brain. Lipophilic statins (simvastatin, lovastatin, atorvastatin) cross the blood-brain barrier more effectively than hydrophilic ones. The choice of statin matters for any potential anti-GBM effect, but dosing to match preclinical concentrations may not always be safe or feasible.
- Drug interactions. GBM patients typically take multiple medications at once — corticosteroids, anti-seizure drugs, temozolomide. Statin interactions with these agents must be evaluated carefully with a prescribing physician.
- No prospective trial-level evidence for GBM survival benefit yet. Current evidence is largely observational and preclinical. Statins cannot be recommended as a standard GBM therapy, and starting them as an anti-cancer strategy without medical supervision carries real risk.
What the Research Horizon Looks Like
The most pressing near-term question is whether statins can be strategically combined with radiation and temozolomide, particularly in patients whose tumors show mevalonate pathway upregulation after treatment. Preclinical models suggest that adding statins to radiation-based protocols may blunt the tumor's post-treatment recovery response, potentially delaying recurrence.
Researchers are also exploring whether specific molecular subtypes of GBM — defined by mutations in IDH, PTEN, or EGFR, for example — are more likely to respond to statins. Finding a predictive biomarker would allow clinicians to select patients most likely to benefit and spare others unnecessary exposure.
Clinical trials investigating statins as adjunct therapy in GBM can be found on ClinicalTrials.gov. If you are considering trial participation, discuss current enrollment opportunities with your neuro-oncologist.
For a broader look at where integrative and adjunct approaches stand in GBM management, see: Integrative Treatments for Glioblastoma: Evidence-Based Complementary Therapies That May Help.
When to Talk to Your Doctor
If you are already taking a statin for cardiovascular disease and have been diagnosed with GBM, tell your neuro-oncologist and cardiologist. They can evaluate whether your current statin type and dose are appropriate alongside your GBM treatment plan.
If you are not on a statin and are wondering whether to start one for a possible anti-tumor effect, do not begin without medical supervision. Statin selection, dose, drug interactions with your current GBM medications, and your kidney and liver function all need to factor into that decision.
Ask your care team: "Are there any open clinical trials evaluating statins alongside my current treatment?" That is the most rigorous and safest way to explore this therapy.
This article is for general information and is not a substitute for medical advice. Always consult your oncologist or care team about your specific situation.