Why Bevacizumab Comes Up at Recurrence
When a glioblastoma grows back after surgery, radiation, and temozolomide, the options shrink fast. Most chemotherapy agents offer little benefit at this stage. Bevacizumab works differently — it targets the blood vessels that feed the tumor rather than the DNA of dividing cancer cells.
It is currently the only FDA-approved targeted therapy specifically for recurrent GBM, so it comes up often in conversations between patients and neuro-oncologists after a first or second relapse. This article explains what bevacizumab does inside a GBM tumor, what the clinical data says about who benefits, and what patients can realistically expect during treatment.
For broader context on why GBM recurs and what your options look like, see our overview on Recurrent GBM: Why It Comes Back, What You Can Do, and How to Navigate What Comes Next.
The Biology: Why GBM Is Such a Vascular Tumor
To understand bevacizumab, you first need to understand one of GBM's defining features: it is one of the most blood-vessel-rich tumors in the human body.
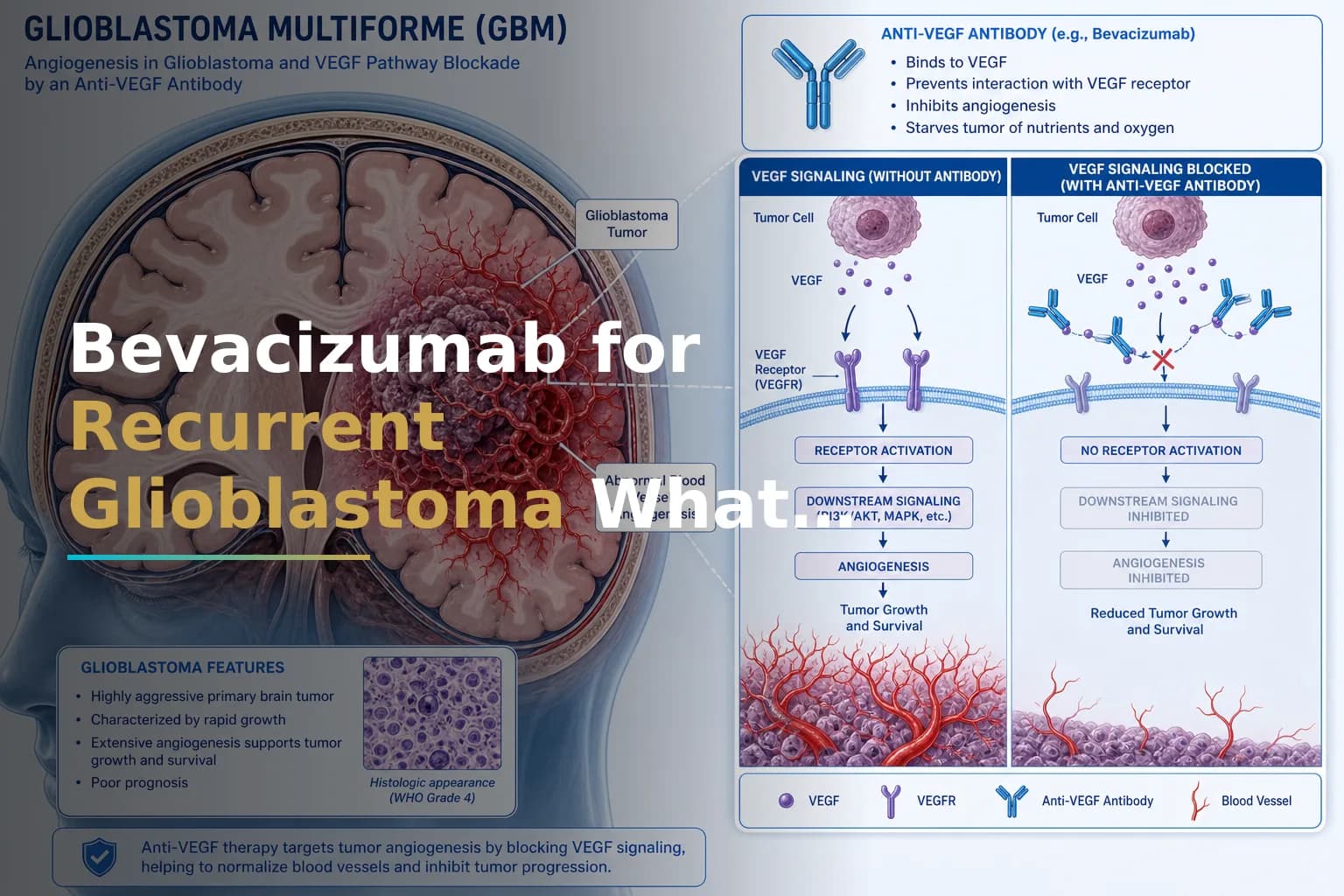
Glioblastoma cells release large amounts of a protein called vascular endothelial growth factor, or VEGF. This protein signals the body to build new blood vessels into the tumor — a process called angiogenesis. Those vessels supply the tumor with oxygen and nutrients it needs to grow and invade surrounding brain tissue.
Glioblastomas are highly vascularized cancers with elevated expression levels of VEGF, the dominant mediator of angiogenesis. The vessels these tumors build are also abnormal — leaky and disorganized. That leakiness contributes to cerebral edema (brain swelling), which often drives the most debilitating neurological symptoms patients experience at recurrence.
Bevacizumab is a humanized monoclonal antibody — an engineered immune protein — that binds to VEGF and blocks it from reaching its receptors on blood vessel cells. Its antitumor effects include reducing tumor blood supply, normalizing tumor vasculature, and inhibiting new vessel formation.
One particularly relevant effect: bevacizumab blocks VEGF signaling and reduces vessel leakiness within the brain tumor, triggering a reduction in vasogenic edema and, consequently, lowering corticosteroid requirements. This is the mechanism behind one of its most tangible day-to-day benefits — reducing dependence on steroids like dexamethasone.
FDA Approval: What the Pivotal Trials Showed
Bevacizumab's path to FDA approval for recurrent GBM moved in two stages.
The key data came from the phase II BRAIN study. In the single-agent bevacizumab arm, tumor responses were observed in 26% of the 85 patients treated with bevacizumab alone, and the median duration of response was 4.2 months. All enrolled patients had already received temozolomide and radiation, so this was a true second-line population.
Years later, bevacizumab received full FDA approval, converting from the accelerated pathway. This regular approval was based on the totality of evidence, including the phase III EORTC 26101 trial, in which adding bevacizumab to lomustine chemotherapy failed to improve overall survival — the primary endpoint — but did improve progression-free survival, a secondary endpoint, compared to lomustine alone.
That distinction matters. The EORTC 26101 trial enrolled 432 patients at first disease progression after standard radiotherapy and temozolomide. It is the largest randomized trial in this setting, and its results shape how clinicians think about what bevacizumab can and cannot do.
What Bevacizumab Actually Does — and Does Not Do
Looking at the evidence clearly is essential for making an informed decision. The data points in different directions depending on which outcome you examine.
Where evidence is positive
- Tumor response rate: A 2021 systematic review and meta-analysis of five randomized controlled trials covering 807 patients found that bevacizumab provided a significantly improved objective response rate (relative risk 2.67) and a modest but statistically significant improvement in median progression-free survival (approximately 1.1 additional months) compared to standard treatments.
- Steroid reduction: In the BRAIN study, 16 out of 86 patients on dexamethasone were able to discontinue the steroid completely, and an additional 33 had a sustained reduction in corticosteroid use after bevacizumab. This matters because long-term steroid use carries significant risks, including muscle wasting, immune suppression, blood sugar problems, and bone loss.
- Radiographic response: Bevacizumab often produces clear reductions in gadolinium-enhancing lesions on MRI. This can appear as dramatic tumor shrinkage on scans, which may allow some patients to maintain or regain neurological function.
- Quality of life signals: A single-institution retrospective study found that the median steroid dose dropped by over 90% in bevacizumab-treated patients two months after starting therapy, and the independent living score — a validated measure of patient independence — was nearly double in the bevacizumab group compared to untreated patients.
Where evidence is more limited
- Overall survival: Across multiple randomized trials, bevacizumab has not been shown to extend how long patients live overall. The same meta-analysis cited above found no statistically significant improvement in median overall survival. This is the most important caveat and one your oncology team will likely discuss with you directly.
- Post-bevacizumab options narrow: Once a tumor progresses on bevacizumab, treatment options become very limited. There is no consensus on what to do next. Many clinical trials also exclude patients who have already received bevacizumab, which is a practical consideration when deciding when to use it.
- Pseudo-response on MRI: Bevacizumab strongly reduces the contrast enhancement visible on standard MRI — partly by sealing leaky vessels rather than killing tumor cells. This can make it hard to tell whether the tumor is truly responding or whether the drug has simply changed how vessels appear on imaging. This is a recognized challenge in neuro-oncology and part of why distinguishing true tumor activity from treatment-related imaging changes requires specialized MRI sequences and expert radiological review.
Who Tends to Respond Better
Research has begun to identify features that may predict a better response to bevacizumab, though no definitive biomarker has been validated for clinical use yet.
A large scoping review found that specific molecular alterations — particularly IDH mutation status — and clinical features such as large tumor burden may predict better responses to bevacizumab treatment. IDH-mutant GBMs, which are less common and generally carry a better baseline prognosis, appeared to show more benefit in some analyses.
The same review found that combining bevacizumab with other treatments, especially lomustine or tumor-treating fields (TTFields), may produce better outcomes than bevacizumab alone. Your molecular profile — including MGMT methylation status, IDH status, and EGFR amplification — is relevant here. Our guide on understanding your GBM molecular profile explains what these markers mean and why they matter at recurrence.
Patients with larger areas of enhancement before treatment often show more visible MRI response, since there is more room for the drug's anti-edema effects to register. Functional status also matters: bevacizumab may offer a stabilizing benefit for patients experiencing acute neurological decline, helping someone who might otherwise not be considered eligible for further therapy.
How Bevacizumab Is Given
Bevacizumab is given intravenously at an infusion center, not taken by mouth. It is given on a cycle schedule — typically every two weeks. The infusion takes between 30 and 90 minutes depending on whether it is a first or subsequent dose. Treatment continues until the tumor progresses on imaging or side effects become unacceptable.
It may be given alone or combined with chemotherapy. The phase III EORTC 26101 trial studied its combination with lomustine (CCNU). Other combinations — including with temozolomide, irinotecan, and investigational agents — have been studied in phase II trials with mixed results.
Side Effects: What to Watch For
Bevacizumab generally has manageable toxicity compared to many chemotherapy agents, but its side effects are distinct and require monitoring.
The most common side effects include:
- High blood pressure (hypertension): This is the most frequently observed adverse event. Patients treated with bevacizumab showed significantly higher rates of grade 3/4 hypertension compared with standard treatments. Blood pressure is checked before each infusion. Some research suggests that developing hypertension may signal the drug is working, making it a potential marker of response.
- Proteinuria: The kidneys may leak protein into the urine. Routine urinalysis is done to track this.
- Fatigue: One of the most commonly reported symptoms, though it can be hard to separate from disease-related fatigue.
- Impaired wound healing: Bevacizumab can slow tissue repair. For this reason, it is typically paused for several weeks before and after any surgical procedures.
- Thromboembolism: Blood clots in the veins are a recognized risk. Deep vein thrombosis and pulmonary embolism have been reported in clinical trials.
- Hemorrhage (bleeding): Because bevacizumab affects blood vessel integrity, there is a small but real risk of intracranial or gastrointestinal bleeding. The FDA label carries boxed warnings for gastrointestinal perforation, wound healing complications, and hemorrhage.
Severe side effects occur in a minority of patients, but your care team will monitor you closely. Report new headaches, vision changes, leg swelling, or sudden neurological changes right away.
Bevacizumab and Resistance: What Happens When It Stops Working
One of the hardest aspects of bevacizumab therapy is what happens when the tumor eventually escapes it. Resistance to bevacizumab can develop and can lead to a pattern of disease progression characterized by non-enhancing disease on MRI imaging. This means the tumor may begin growing differently — spreading through brain tissue without forming the leaky, contrast-enhancing vessels the drug was designed to block.
This non-enhancing growth pattern is harder to detect on standard imaging and may show up as subtle cognitive changes rather than the classic mass effect. FLAIR sequences on MRI are important for tracking it. Researchers are studying resistance mechanisms — including alternative angiogenic pathways, immune cell infiltration, and hypoxia-driven tumor adaptation — to find combinations that could extend bevacizumab's benefit or overcome resistance.
When bevacizumab stops working, the remaining options are limited. This is why many neuro-oncologists recommend that patients look into clinical trial eligibility before starting bevacizumab, to preserve the widest possible access to novel agents. Emerging approaches such as CAR-T cell therapy are active areas of study in this post-bevacizumab setting.
Combining Bevacizumab With Other Approaches
Research continues to explore whether bevacizumab works better as part of a combination strategy. Current evidence favors:
- Bevacizumab plus lomustine: This combination has the strongest phase III evidence base (EORTC 26101) and was part of the basis for full FDA approval. It did not improve overall survival but did improve tumor response rates compared to lomustine alone.
- Bevacizumab plus tumor-treating fields (TTFields): Emerging data suggests this combination may improve outcomes at recurrence, though strong randomized evidence is still limited.
- Earlier use at first recurrence: Some analyses suggest using bevacizumab at first recurrence — rather than later relapses — may produce better outcomes, though the optimal timing has not been definitively established.
Combinations with immunotherapy agents, including checkpoint inhibitors, have largely disappointed in phase II trials. The broader immunotherapy landscape in GBM remains an active research area, and there is interest in whether bevacizumab's vascular-normalizing effect could one day help immune cells penetrate the tumor more effectively.
Integrating Bevacizumab Into a Broader Recurrence Strategy
Bevacizumab is one tool in a broader plan. Most experienced GBM teams approach recurrence by considering:
- Whether re-surgery or re-irradiation is feasible
- Eligibility for clinical trials that might offer access to novel agents
- Molecular profile findings that might point toward off-label options (see our articles on tamoxifen and paxalisib for MGMT-unmethylated GBM for examples)
- Supportive care goals, including steroid reduction, symptom management, and quality of life
The question of whether bevacizumab should come before or after clinical trial participation matters. Some trials exclude patients who have already received bevacizumab. Talking through this sequence with a neuro-oncologist — ideally at a comprehensive cancer center — before committing to any one path is strongly advisable.
When to Talk to Your Doctor
Bevacizumab is a reasonable, FDA-approved option to discuss with your neuro-oncologist when GBM recurs after standard treatment. The conversation should include honest expectations — including the absence of an established overall survival benefit in phase III trials — alongside its real practical advantages in symptom control and steroid reduction. Ask about clinical trial eligibility before starting, discuss your molecular profile and whether it predicts a stronger or weaker response, and understand the monitoring plan for blood pressure, urine protein, and imaging. Every patient's situation is different, and what makes sense for one person may not be right for another.
This article is for general information and is not a substitute for medical advice. Always consult your oncologist or care team about your specific situation.