Why Repurpose an Antimalarial Drug for Brain Cancer?
Drug repurposing means taking a medication already approved for one condition and testing it against another. The appeal is straightforward: the drug's safety profile is known, costs are lower, and the path to clinical use may be faster. For glioblastoma (GBM) — a tumor where standard treatment still leaves most patients facing recurrence — researchers have been mining existing drug libraries for new options.
Chloroquine (CQ) and its close relative hydroxychloroquine (HCQ) have attracted serious scientific attention in this space. There is growing evidence that the antimalarial chloroquine could be repurposed for cancer treatment, and a dozen clinical trials have been initiated over the past decade to test its potential as an adjuvant treatment for therapy-refractory cancers, including glioblastoma. This page breaks down what the science actually says — and what it does not yet say — so you can have an informed conversation with your neuro-oncologist.
For broader context on how metabolic and repurposed drugs are being explored in GBM, see our overview of integrative treatments for glioblastoma and our deep-dive on metformin as another repurposed drug candidate.
What Is Autophagy — and Why Does It Matter in GBM?
The word "autophagy" comes from Greek and means "self-eating." It is the cell's built-in recycling system. When a cell is stressed — by low oxygen, nutrient shortage, or toxic therapy — autophagy breaks down damaged proteins and organelles, packages them in membrane sacs, and sends them to the lysosome to be degraded and reused.
Autophagy is a catabolic pathway that delivers cellular components sequestered into vesicles for lysosomal degradation, and it plays an important role in maintaining cellular homeostasis — becoming upregulated during stress conditions such as limited nutrient and oxygen availability, and in response to anti-cancer therapy.
In GBM, this process has a dark side. Glioblastoma engages multiple survival mechanisms, including autophagy, and GBM exploits both degradative and secretory autophagy pathways to support tumor growth and limit the efficacy of standard-of-care treatments. In plain terms: GBM cells activate autophagy as a shield, using it to stay alive when radiation and temozolomide try to kill them.
In glioma cells, autophagy has been demonstrated to be an adaptive response to both radiation and temozolomide (TMZ), suggesting that inhibition of autophagy could have therapeutic benefit. That is the core logic driving interest in chloroquine.
The biology has a complication, though. Paradoxically, autophagy in cancer can promote either cell death or cell survival, and the effect of autophagy in glioblastoma during tumor initiation, promotion, and progression is still controversial, given its regulatory role in both cell death and survival. This dual nature helps explain why clinical trial results have been mixed.
How Chloroquine Blocks Autophagy
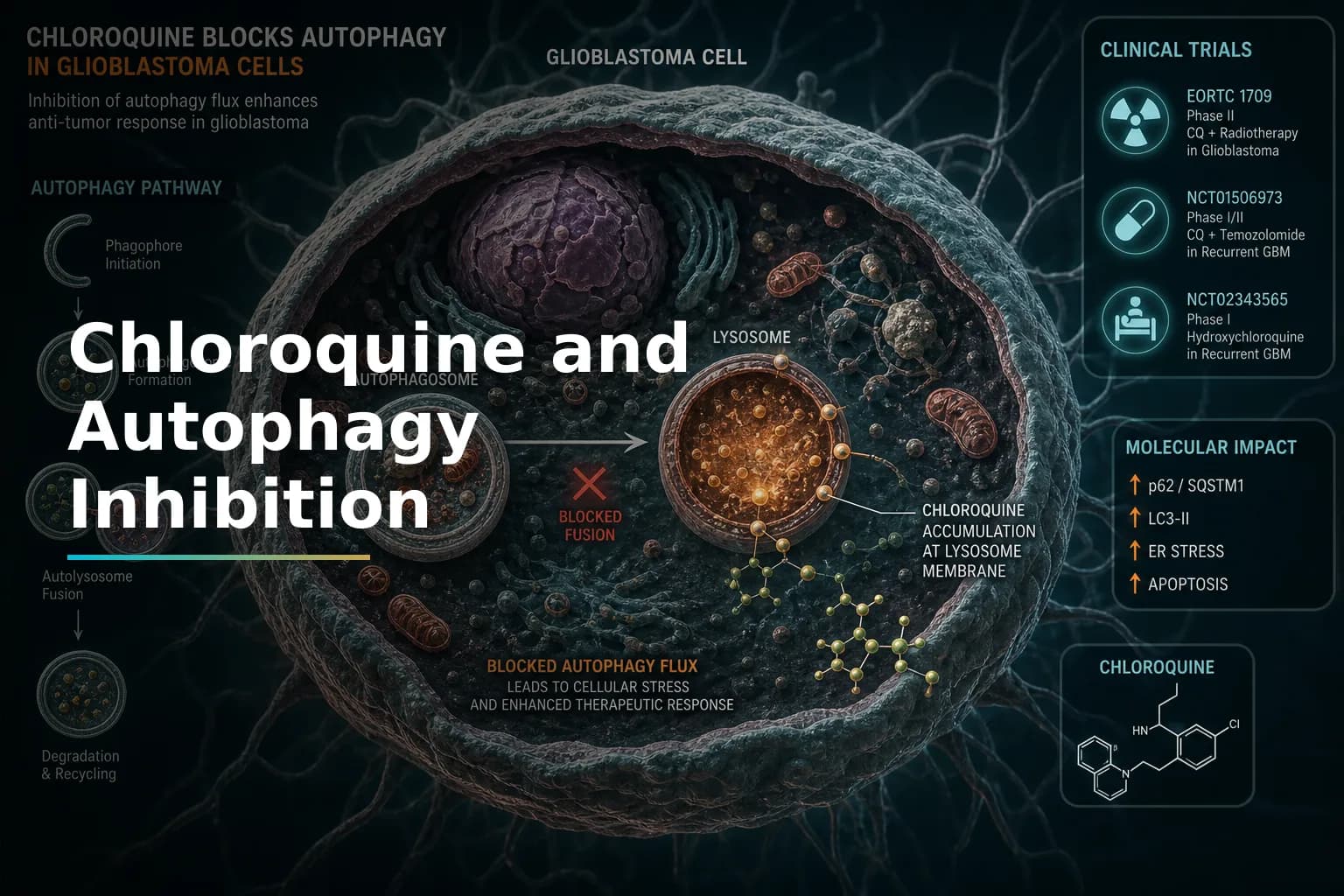
Chloroquine is classified as a lysosomotropic agent. That means it concentrates inside lysosomes — the cell's digestive compartments. Chloroquine (CQ) is a 4-aminoquinoline commonly used for the prophylaxis and treatment of malaria, rheumatoid arthritis, and other conditions. It accumulates in the lysosome and thereby raises the intralysosomal pH, preventing the autophagosome-lysosome fusion essential for autophagy.
When that fusion is blocked, the cell can no longer complete the recycling process. Damaged components pile up and the tumor cell's stress-response toolkit is weakened. In theory — and in preclinical models — this makes the cell more vulnerable to the DNA damage caused by radiation and temozolomide.
Treatment of glioblastoma xenografts with chloroquine results in autophagy inhibition, leading to a reduction of tumor hypoxia and sensitization to radiation. Hypoxic (low-oxygen) regions deep inside a GBM tumor are notoriously resistant to radiotherapy. Reducing hypoxia by blocking autophagy could make radiation more effective, at least in laboratory models.
Researchers have also noted a potential molecular target. Preclinical data suggest that EGFRvIII-expressing glioblastoma may benefit most from chloroquine because of autophagy dependency. EGFRvIII is a mutant form of the epidermal growth factor receptor found in a subset of GBM tumors. If confirmed in trials, this could help identify which patients are most likely to respond. To learn more about molecular markers like EGFR, see our article on understanding your GBM molecular profile.
Beyond autophagy, researchers are finding other mechanisms at play. Up until recently, inhibition of the late stage of autophagy was thought to be the major mechanism of chloroquine-mediated cancer cell death. However, recent research has provided compelling evidence that autophagy-inhibiting activities of chloroquine are dispensable for its ability to suppress tumor cell growth. This means the drug may have additional anti-tumor effects that are still being studied.
What Do the Clinical Trials Actually Show?
This is where expectations need to be calibrated. Trial results range from intriguing to inconclusive.
Early Randomized Studies: Promising but Small
In a double-blind, placebo-controlled trial, patients younger than 60 years received standard chemo-radiotherapy with or without 12 months of chloroquine. The median overall survival was 24 months for those given chloroquine but 11 months with placebo (hazard ratio 0.52, p = .14). A separate non-blinded randomized trial showed a marked increase in survival (median 33 months with chloroquine vs. 11 months without, p < .001).
Those numbers look striking. But there is an important caveat: these were small, single-center studies conducted before the Stupp protocol (temozolomide + radiation) became standard of care. Being done at the same institution also limits how broadly the results apply.
The Phase I/II HCQ Trial (ABTC 0603)
A larger, more rigorous phase I/II study tested hydroxychloroquine added to standard temozolomide and radiation in newly diagnosed GBM patients. The primary objective was to determine the maximum tolerated dose and efficacy of HCQ in combination with radiation therapy and temozolomide. A 3+3 phase I trial design followed by a noncomparative phase II study was conducted in GBM patients after initial resection, with patients receiving HCQ orally each day alongside radiation and concurrent and adjuvant temozolomide.
The phase II cohort (n = 76) had a median survival of 15.6 months, with survival rates at 12, 18, and 24 months of 70%, 36%, and 25%. These results did not differ significantly from outcomes expected with standard care alone at the time of the trial.
The key finding: These data establish that autophagy inhibition is achievable with HCQ, but dose-limiting toxicity prevented escalation to higher doses; at HCQ 600 mg/day, autophagy inhibition was not consistently achieved, and no significant improvement in overall survival was observed. In short, the drug worked as a biological tool — it did inhibit autophagy in patients — but not consistently enough at safe doses to produce a clear survival benefit.
The CHLOROBRAIN Phase IB Trial
The CHLOROBRAIN study explored the safety, pharmacokinetics, and maximum tolerated dose of chloroquine in combination with radiotherapy and concurrent daily temozolomide in patients with newly diagnosed GBM, using a single-centre, open-label, dose-finding phase I design where patients received oral chloroquine once daily one week before concurrent chemoradiation.
A daily dose of 200 mg chloroquine was established as the maximum tolerated dose when combined with radiotherapy and concurrent temozolomide for newly diagnosed GBM. Favorable tolerability and extensive pre-clinical evidence on anti-tumor activity were cited as support for further phase II and III studies.
Where Does the Field Stand Now?
In addition to glioma, chloroquine is currently being investigated in a wide range of cancer types, with studies recruiting including a large phase III trial in glioma (NCT03243461). Phase III trials are the gold standard — they test whether a drug actually extends survival in a randomized, controlled setting. Results from these larger trials will be critical to understanding whether chloroquine has a real role in GBM care.
A definitive test of the role of autophagy inhibition in the adjuvant setting for glioma patients awaits the development of lower-toxicity compounds that can achieve more consistent inhibition of autophagy. That statement, from a major trial team, captures where the field is today: the hypothesis is solid, but the tools to test it fully are still being refined.
Known Risks and Side Effects
Chloroquine and HCQ are generally well-tolerated at standard doses for malaria or autoimmune disease. Their use in oncology — often at higher doses — raises specific concerns that patients need to understand.
Retinal Toxicity
The most serious long-term risk is damage to the retina. Hydroxychloroquine and chloroquine have been associated with irreversible visual loss due to retinal toxicity. Hydroxychloroquine retinal toxicity is far more common than previously considered, with an overall prevalence of 7.5% identified in patients taking HCQ for greater than 5 years, rising to almost 20% after 20 years of treatment.
At the higher doses sometimes used in oncology trials, the risk window is shorter. Patients receiving HCQ at 800 to 1000 mg/day showed a 25% to 40% incidence of retinopathy and signs of damage within 1 to 2 years. Most GBM trials use lower doses and shorter durations, but ophthalmologic monitoring is essential for anyone taking these drugs.
Retinal toxicity from hydroxychloroquine is rare at standard doses, but even if the medication is discontinued, vision loss may be irreversible and may continue to progress. Before treatment is initiated with hydroxychloroquine, a complete ophthalmic examination should be performed to determine any baseline maculopathy.
Other Common Side Effects
- Gastrointestinal: Nausea, abdominal cramps, and diarrhea are reported in a meaningful minority of patients. In one breast cancer window-of-opportunity trial, nearly 15% of patients discontinued treatment due to adverse events, mainly nausea and/or abdominal cramps.
- Cardiac: QT interval prolongation can occur, particularly at higher doses or when combined with other QT-prolonging medications.
- Neurological: Headache, dizziness, and in rare cases, neuromuscular effects have been reported.
- Dermatological: Skin reactions, including rashes, may occur.
Chloroquine also has an unusually long half-life of 40–60 days, meaning it stays in the body long after a dose is stopped. This extensive plasma terminal elimination half-life means potential for long-term toxicity even after treatment ends. Any trial or off-label use requires careful medical supervision for an extended period.
Chloroquine vs. Hydroxychloroquine: What Is the Difference?
HCQ is a chemical derivative of CQ. Hydroxychloroquine was developed through the chemical addition of a hydroxyl group and was established as a systemically less toxic alternative to chloroquine in the 1940s–50s. In practice, both drugs inhibit autophagy through the same mechanism. HCQ is now more commonly studied in cancer trials because its lower toxicity allows more flexibility in dosing — though dose-limiting toxicity has still been a challenge in GBM studies.
Chloroquine has been used for 60 years in humans for malaria prophylaxis and treatment, rheumatoid arthritis, and HIV, and it is an inexpensive, orally available drug that has central nervous system penetration. CNS penetration matters here — many drugs fail against brain tumors because they cannot cross the blood-brain barrier in useful concentrations.
What the Evidence Does Not Yet Show
It is worth being clear about the limits of current knowledge:
- No large, randomized, phase III trial has conclusively shown a survival benefit for chloroquine or HCQ added to standard GBM care in newly diagnosed patients.
- Phase I/II trial results confirm the drug inhibits autophagy in the body, but consistent inhibition at safe doses has not been reliably achieved.
- It is not yet known which molecular subtypes of GBM — beyond EGFRvIII — are most likely to respond. Tumor heterogeneity makes this question difficult.
- The best timing, dose, and duration for combining these drugs with temozolomide and radiation has not been established.
This is not a reason to dismiss the approach. It is a reason to direct interest toward rigorous clinical trials rather than unmonitored self-treatment.
Exploring Trials: How to Find Open Studies
Patients and caregivers researching chloroquine or HCQ for GBM should search ClinicalTrials.gov directly. Use search terms such as "glioblastoma hydroxychloroquine," "GBM chloroquine," or "autophagy inhibition brain tumor." Filter by "Recruiting" status and check eligibility criteria carefully — prior treatments, MGMT methylation status, and EGFR status often affect who qualifies.
Key questions to bring to your neuro-oncologist or trial coordinator:
- Is my tumor's molecular profile (EGFRvIII, MGMT status) relevant to any open CQ/HCQ trial?
- Would adding an autophagy inhibitor conflict with my current or planned treatments?
- What ophthalmologic monitoring would be required?
- Are there combination trials pairing CQ/HCQ with other repurposed agents or immunotherapies?
For a broader look at the trials landscape in GBM, see our article on recurrent GBM: what comes next. If you are interested in how metabolic approaches connect to autophagy biology, our article on the ketogenic diet and glioblastoma covers related mechanisms.
When to Talk to Your Doctor
Raise the topic of chloroquine or hydroxychloroquine with your neuro-oncologist if you are actively researching trial options, are interested in drug repurposing strategies, or have a tumor profile with EGFRvIII amplification or other features that may affect trial eligibility. Do not obtain or use these drugs outside of a supervised medical setting. Both carry real toxicity risks — particularly to vision — that require professional monitoring.
This article is for general information and is not a substitute for medical advice. Always consult your oncologist or care team about your specific situation.