When the MRI Changes — But It May Not Be the Tumor
You finished radiation and chemotherapy for glioblastoma. You go in for your follow-up MRI. The scan shows a new area of enhancement or a growing lesion. Your first thought is almost certainly: the tumor is back.
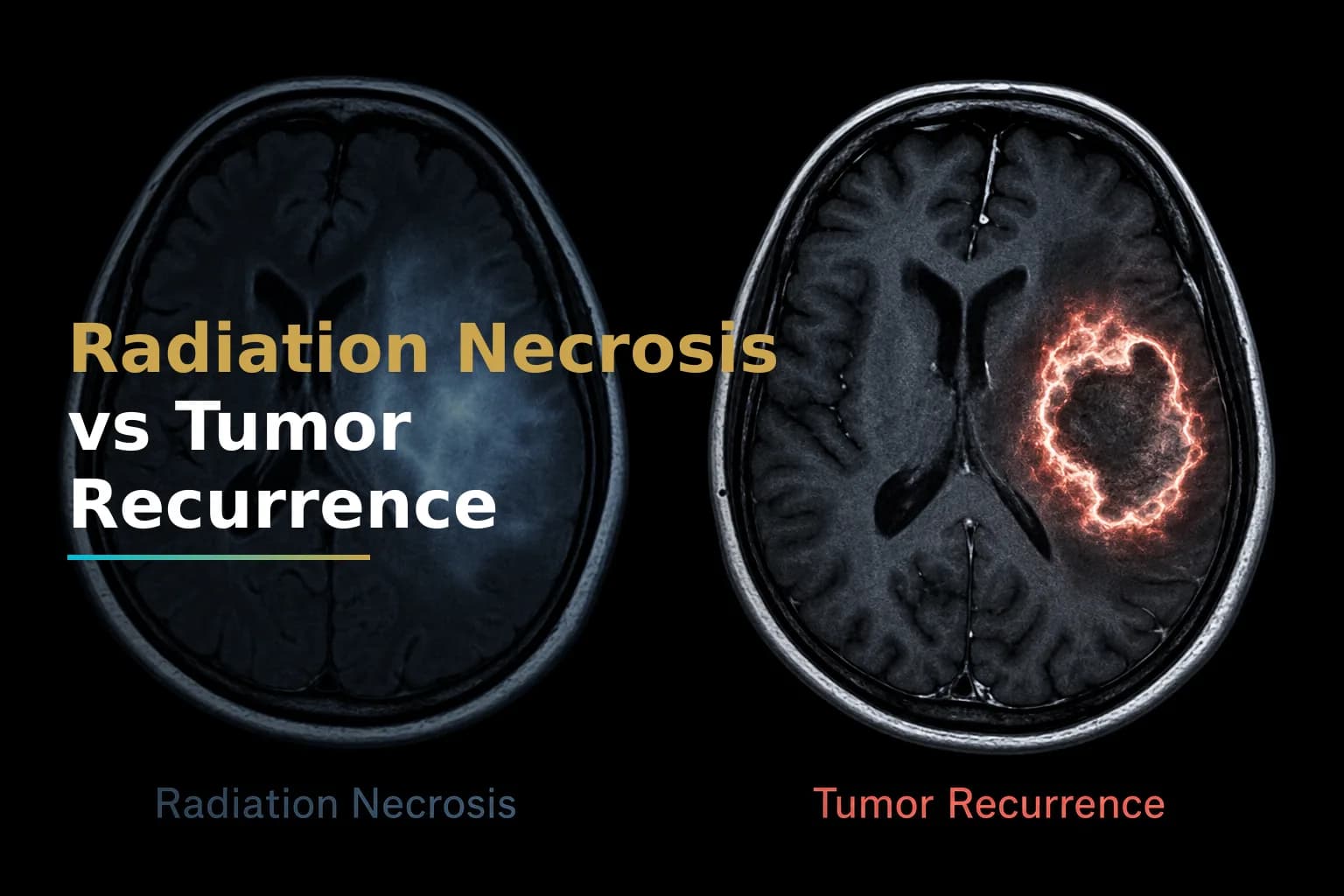
But that is not always what the image means. A condition called radiation necrosis can produce MRI findings that look nearly identical to tumor recurrence. It is caused by treatment, not by the tumor itself, and it requires a completely different management approach.
Telling radiation necrosis apart from true tumor recurrence is one of the most consequential diagnostic challenges in glioblastoma care. Getting it wrong can mean unnecessary surgery, delayed treatment, or changed chemotherapy that was never needed.
This article explains what radiation necrosis is, why it happens, how doctors try to distinguish it from recurrence, and what your options are if it is confirmed.
What Is Radiation Necrosis?
Radiation necrosis (RN) is the death of brain tissue caused by radiation damage. It is not cancer. It happens because ionizing radiation, while effective at destroying tumor cells, can also injure the blood vessels and supporting structures of the surrounding healthy brain tissue.
At a cellular level, radiation-associated neurotoxicity involves vascular injury, glial and white matter damage, and disruption of the fibrinolytic enzyme system. In chronic radiation injury, endothelial damage leads to vascular dilation, thickened vessel walls, and increased capillary permeability, which produces the edema visible on imaging. Pathologically, radiation necrosis tissue is largely paucicellular, meaning it contains very few living cells, and it is surrounded by gliotic (scarred) brain tissue.
Radiation necrosis is considered a late complication of radiotherapy. It occurs in approximately 5%–10% of patients who have undergone radiotherapy. Early cases may appear within months of finishing radiation, while late-onset necrosis can develop several years post-treatment.
How Does It Differ From Pseudoprogression?
You may have heard the term pseudoprogression from your care team. It is related but distinct.
Pseudoprogression refers to MRI changes — typically contrast enhancement — that appear in the early weeks to months after completing chemoradiation and then stabilize or improve on their own. It is usually asymptomatic. In contrast, radiation necrosis may appear months to several years after radiation therapy and involves a space-occupying necrotic lesion with mass effect and neurological dysfunction.
MGMT methylation status is relevant here. Patients with MGMT-methylated tumors appear to have a higher rate of pseudoprogression after chemoradiation with temozolomide. If you are unsure about your molecular profile, our article on Understanding Your GBM Molecular Profile: IDH, MGMT, EGFR & Why They Matter explains how these markers are used in treatment decisions.
True radiation necrosis tends to be more persistent and more symptomatic than pseudoprogression. Both can mimic tumor recurrence and require careful monitoring.
Why Does Glioblastoma Treatment Increase the Risk?
Standard glioblastoma treatment involves maximal safe surgical resection followed by concurrent radiation plus temozolomide chemotherapy. This combination is highly effective, but it also makes follow-up imaging harder to interpret.
Several studies found more frequent radiation necrosis without evidence of true progression in glioblastoma patients undergoing combined chemoirradiation with temozolomide. In one series of 51 glioblastoma patients, 26 showed radiological progression within the first 6 months after completing radiotherapy — and in 15 of those 26 patients, histological evaluation showed only necrosis, not tumor.
Adding chemotherapy to radiation appears to change both the incidence and timing of these treatment-related imaging changes, making them harder to interpret.
Symptoms: What Does Radiation Necrosis Feel Like?
This is part of what makes radiation necrosis so difficult to detect on clinical grounds alone. Its symptoms overlap significantly with those of tumor recurrence.
Symptoms may include:
- Headaches
- Seizures
- Focal neurological deficits (weakness, speech problems, vision changes)
- Cognitive changes or memory difficulties
- Fatigue
- Altered mental status
These symptoms depend on where in the brain the necrosis is located. Some patients have very mild or no symptoms at all, while others experience significant neurological decline. Symptom severity does not reliably predict whether the cause is necrosis or true tumor.
The Diagnostic Challenge: Why Standard MRI Is Not Enough
On conventional MRI, radiation necrosis appears as an enlarging, contrast-enhancing mass with surrounding edema — almost identical to tumor recurrence. Radiation necrosis often manifests as an enhancing mass lesion with varying degrees of surrounding edema and progressive enhancement on serial MRI.
Standard T1 post-gadolinium and T2/FLAIR sequences alone cannot reliably distinguish between the two. This is why neuro-oncology teams use advanced imaging tools and, in some cases, tissue sampling.
Advanced Imaging Techniques
Several imaging modalities have shown value in distinguishing radiation necrosis from tumor recurrence:
- Perfusion MRI (DSC-PWI): Measures blood flow through the lesion. Actively growing tumor tends to have higher relative cerebral blood volume (rCBV), while radiation necrosis typically shows lower perfusion. Multiparametric MRI combining several perfusion parameters is a valuable noninvasive tool for discriminating tumor recurrence from radiation necrosis.
- MR Spectroscopy (MRS): Analyzes the chemical composition of tissue. Tumor recurrence often shows elevated choline (a marker of cell membrane turnover) and reduced NAA (a neuronal health marker), while necrosis shows different metabolite patterns.
- Diffusion-Weighted Imaging (DWI) and Diffusion Tensor Imaging (DTI): Measures how water molecules move through tissue. These can help differentiate the cellular density differences between active tumor and necrotic tissue.
- PET Imaging: Radiolabeled amino acid PET tracers (such as FET or MET) are more specific for brain tumors than standard FDG-PET and can help detect active tumor metabolism distinct from necrotic tissue.
- Radiomics and AI-based models: Research teams are combining MRI features into integrated diagnostic models. One study combining radiomics with PET data showed promising accuracy in distinguishing the two conditions at the population level, though individual patient application is still evolving.
Even with these tools, none provides absolute certainty, and conflicting results across modalities are common.
Biopsy: The Gold Standard
When imaging remains inconclusive, tissue biopsy is the most definitive path forward. Currently, the only definitive way to distinguish between radiation necrosis and recurrent tumor is through surgical intervention followed by thorough histopathological evaluation.
Under the microscope, radiation necrosis tissue is largely paucicellular with increased water in the interstitial spaces. Recurrent tumor, by contrast, contains viable tumor cells with pleomorphic nuclei and dense cytoplasmic processes — it is highly cellular with a high nuclei-to-cytoplasm ratio. Even biopsy has limits, though: mixed histology with both necrosis and viable tumor in the same sample is common and may not tell the full story.
Surgery can also serve a dual purpose: it allows tissue diagnosis and can relieve mass effect from the necrotic lesion itself. For patients with surgically accessible lesions and symptoms from mass effect, reoperation may be both diagnostic and therapeutic. For more on what recurrence evaluation looks like, see our article on Recurrent GBM: Why It Comes Back, What You Can Do, and How to Navigate What Comes Next.
Treatment Options for Confirmed Radiation Necrosis
Once radiation necrosis is confirmed — or strongly suspected — treatment focuses on managing symptoms, reducing inflammation, and where possible, shrinking the necrotic lesion. There is no single standard protocol, and management is tailored to severity, location, and patient health status.
1. Corticosteroids (First-Line)
Corticosteroids such as dexamethasone are typically the first step. Corticosteroids are traditionally first-line treatment due to their ability to reduce local edema and stabilize vascular permeability. They can provide meaningful symptom relief relatively quickly. However, long-term use carries significant side effects — including blood sugar changes, immune suppression, weight gain, and bone density loss — so they are generally not intended as indefinite therapy.
For patients who do not respond to steroids or cannot tolerate them, additional options are considered.
2. Bevacizumab
Bevacizumab is an anti-VEGF antibody that has become one of the most studied options for radiation necrosis. The rationale is biologically grounded: excessive production of vascular endothelial growth factor (VEGF) from necrotic lesions is a possible mechanism driving radiation necrosis, and the anti-VEGF antibody bevacizumab has been reported as an effective treatment option.
Randomized controlled trials have shown that bevacizumab may reduce necrotic lesions and improve neurological symptoms, including in patients whose necrosis did not respond to steroids. That said, bevacizumab carries its own risks — including effects on blood pressure, wound healing, clotting, and gastrointestinal integrity — and its optimal dosing for radiation necrosis has not been fully established.
Bevacizumab also plays a role in recurrent glioblastoma management. If you are considering it as a salvage option for recurrent disease, the considerations are different. Our article on Recurrent GBM discusses bevacizumab in that context as well.
3. Laser Interstitial Thermal Therapy (LITT)
LITT is a minimally invasive surgical technique in which a laser probe is guided stereotactically into the necrotic lesion to ablate it with heat. It has gained traction for radiation necrosis that does not respond to medical management. Various studies have shown clinical improvement with laser interstitial thermal therapy, and it has been used in addition to surgery to treat radiation brain necrosis.
One meta-analysis comparing LITT to bevacizumab found that LITT provided improved overall survival and similar symptomatic improvement and lesion volume reduction — though LITT may not be feasible for lesions in eloquent brain areas or for patients in poor functional condition.
Early study data suggest neurological improvements and reduced seizure frequency in 50–70% of patients who undergo LITT for radiation necrosis. It also has the advantage of providing tissue for pathological confirmation.
4. Surgery (Resection)
Open surgical resection remains an option for patients with large, symptomatic, accessible necrotic lesions. It can relieve mass effect and allow thorough tissue sampling. However, surgery carries risks including infection, seizures, neurological deficits, and hemorrhage. Even after resection, brain edema may persist for weeks and require close monitoring.
5. Hyperbaric Oxygen Therapy (HBOT)
HBOT delivers pure oxygen at elevated atmospheric pressure, increasing oxygen delivery to oxygen-deprived tissue and potentially promoting healing. Small studies and case reports have shown improvement in a subset of patients, and HBOT may be considered for patients whose necrosis is not well-controlled by other means. However, HBOT is expensive, time-consuming, and not available at all centers. The evidence base is more limited than for bevacizumab or LITT, and it is not universally recommended as a first-line option.
Integrative approaches including HBOT are discussed further in our overview of Integrative Treatments for Glioblastoma: Evidence-Based Complementary Therapies That May Help.
What Happens If It Is a Mix of Both?
Radiation necrosis and tumor recurrence do not always appear in pure form. Mixed pathology — where the same lesion contains areas of necrosis alongside viable tumor cells — is not uncommon. This complicates both diagnosis and treatment planning. In these cases, the clinical team must weigh the relative contribution of each component and design a management strategy accordingly. Multidisciplinary discussion involving neurosurgery, neuro-oncology, radiation oncology, and neuroradiology is essential.
Questions to Ask Your Neuro-Oncology Team
If you or your loved one is facing a new MRI finding after glioblastoma treatment, these questions may help guide your conversation with your care team:
- Is advanced imaging (perfusion MRI, MR spectroscopy, or amino acid PET) available at this center?
- How confident is the team that this represents recurrence versus radiation necrosis, and what is that confidence based on?
- Would tissue biopsy change the treatment plan?
- If radiation necrosis is suspected, what is the first-line management recommendation?
- Are there ongoing clinical trials for radiation necrosis management?
- If the decision is to observe, how often will imaging be repeated?
When to Talk to Your Doctor
Contact your neuro-oncology team promptly if you notice any new or worsening neurological symptoms after completing radiation — including new headaches, changes in speech, weakness, vision changes, or seizures. Do not wait for your next scheduled appointment. New symptoms after treatment require imaging evaluation, and the sooner the team can characterize the finding, the sooner an appropriate plan can be made. If you are in the early period after diagnosis and want to understand what follow-up typically looks like, see our guide on Newly Diagnosed Glioblastoma: What to Expect in the First 30 Days After Diagnosis.
This article is for general information and is not a substitute for medical advice. Always consult your oncologist or care team about your specific situation.