Why Glioblastoma Is a Metabolic Disease — Not Just a Genetic One
Most people think of glioblastoma (GBM) as a genetic problem: mutated DNA, runaway cell growth, failed repair. That picture is accurate, but incomplete. GBM is also a disease of broken energy metabolism, and that broken metabolism may be a therapeutic target you can partly influence through what and when you eat.
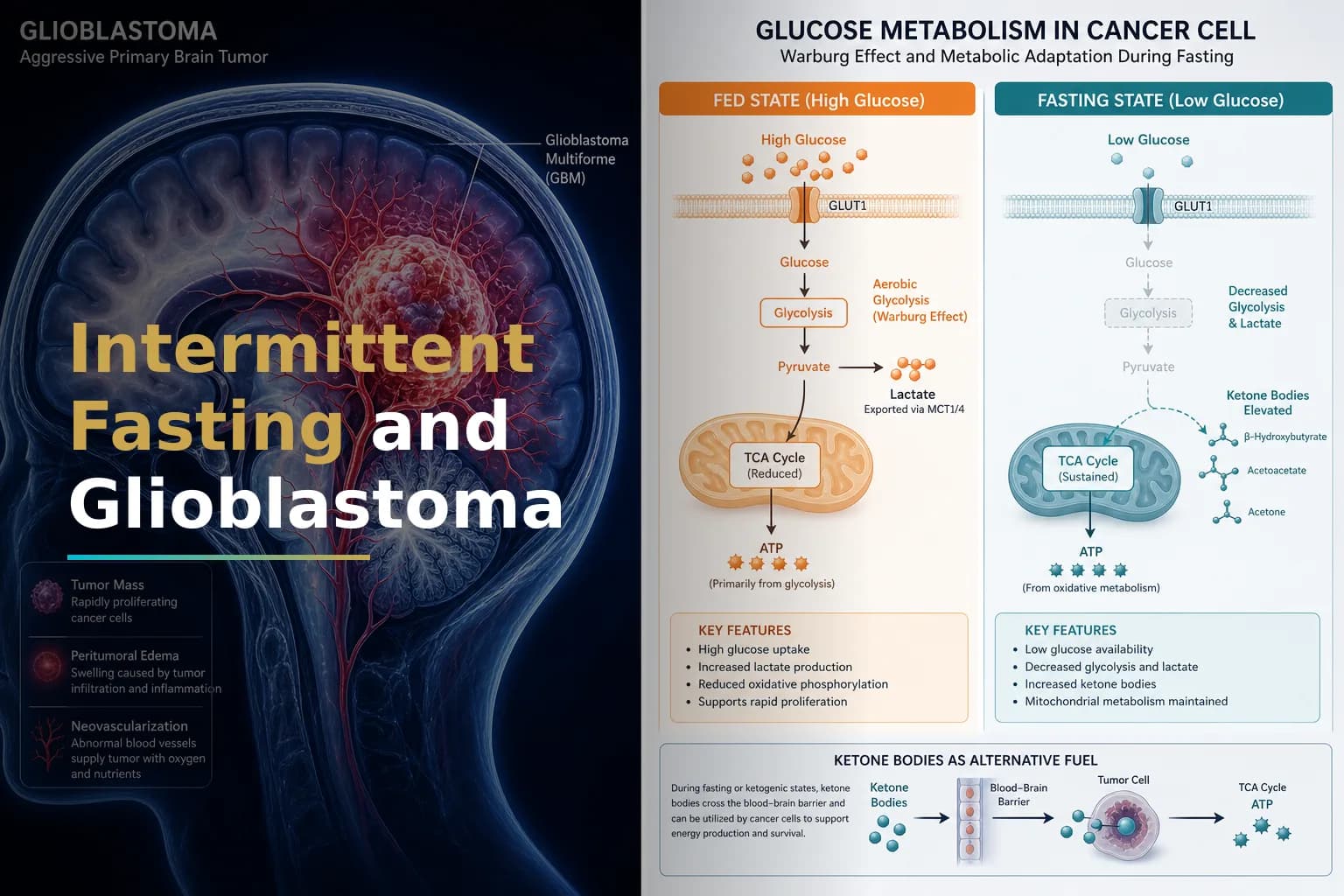
The central concept is called the Warburg effect. More than 90 years ago, Otto Warburg observed that cancer cells burn glucose in a strikingly inefficient way, converting it to lactic acid even when oxygen is plentiful. Research published in PMC confirms that GBM, like most cancers, relies on this aerobic glycolysis — fuelling rapid cell division through high glucose consumption even when oxygen is available.
This is not a minor quirk. A ClinicalTrials.gov-registered metabolic therapy trial summarizes the core idea clearly: most GBM cells have damaged mitochondria and rely almost exclusively on glucose for energy, while normal brain cells can also use fatty acids and ketone bodies. That difference creates a potential metabolic vulnerability. Strategies that reduce blood glucose and raise ketones may stress tumor cells more than healthy tissue.
This is where intermittent fasting (IF) and caloric restriction (CR) enter the picture. Both approaches lower circulating glucose and insulin, raise ketone bodies, and reduce levels of insulin-like growth factor 1 (IGF-1) — a growth-signaling protein that tumors exploit. The question is whether these shifts translate into real clinical benefit for GBM patients.
What Intermittent Fasting Actually Does in the Body
Intermittent fasting is not a single diet. It is a family of eating patterns that cycle between periods of eating and periods of fasting or very low calorie intake. Common forms include:
- Time-restricted eating (TRE): Limiting food intake to a set window, typically 6–10 hours per day.
- Alternate-day fasting: Alternating normal eating days with very low calorie days (around 500 kcal).
- Periodic fasting: Extended fasts of 24–72 hours, sometimes timed around chemotherapy cycles.
- Fasting-mimicking diets (FMD): Very low calorie, plant-based protocols designed to trigger fasting biology without complete abstinence from food.
Each approach produces overlapping physiological changes: lower blood glucose, lower insulin, lower IGF-1, higher ketones, and activation of cellular stress-response pathways like autophagy. For GBM patients, the most studied combination is fasting paired with a calorie-restricted ketogenic diet.
Related reading: The Ketogenic Diet and Glioblastoma: What the Evidence Actually Says About Using Metabolic Therapy Alongside Standard Treatment
The "Differential Stress Resistance" Hypothesis
One compelling idea in fasting research is called Differential Stress Resistance (DSR). Developed partly through glioma-specific studies, it proposes that fasting protects healthy cells from chemotherapy toxicity while leaving cancer cells — locked into a growth-driven metabolism — more vulnerable.
A preclinical study published in PMC tested this directly in glioma models. In cell culture, starvation-mimicking conditions sensitized mouse, rat, and human glioma cells — but not normal glial cells — to temozolomide (TMZ). In live animal models, 48 hours of fasting significantly reduced blood glucose and circulating IGF-1, and sensitized both subcutaneous and intracranial glioma tumors to radio- and chemotherapy, extending survival in the mouse models tested.
The same research group found that the mechanism partly depends on IGF-1. Work published in PMC showed that reducing IGF-1 signaling protected primary glial cells, but not glioma cells, against cyclophosphamide — directly linking IGF-1 suppression (a consistent effect of fasting) to tumor cell vulnerability.
These are preclinical findings in animal models, not human trials. But they form a plausible mechanistic basis for the clinical research now underway.
Key Clinical Trials: What Has Been Tested in GBM Patients
The ERGO and ERGO2 Trials
The most rigorous human data on fasting in GBM comes from the German ERGO trial series. The ERGO2 trial, published in the European Journal of Nutrition via PMC, was a prospective, randomized study that tested a combined calorie-restricted ketogenic diet and intermittent fasting (KD-IF) protocol alongside re-irradiation for recurrent glioblastoma. Fifty patients were randomized 1:1.
The trial did not meet its primary endpoint of improved progression-free survival compared to standard diet. However, the investigators raised important methodological questions. The nine-day intervention window may have been too short. The higher-calorie days built into the ketogenic diet phase may have interfered with fasting's known effects on IGF-1, glucose, and insulin. The researchers also noted that ketone bodies were detectable in tumor tissue in only 4 of 11 patients assessed — suggesting the intervention did not reliably achieve its intended metabolic state in all participants.
The authors concluded that repeated fasting cycles during first-line therapy — rather than a single brief episode at recurrence — might produce a stronger effect on tumor metabolism. This is a useful finding for how future trials should be designed.
The Metabolic Therapy Program (MTP) Trial
A registered trial at ClinicalTrials.gov (NCT04730869) is evaluating a metabolic therapy program using fasting and ketogenic diets alongside standard GBM treatment. The rationale is straightforward: metabolic interventions target cancer cell metabolism by lowering blood glucose and raising ketones, creating an advantage for normal cells and a disadvantage for cancer cells. Preliminary hospital experience has found the approach feasible and safe in patients with advanced cancer.
Phase 1 Safety and Feasibility Data
A phase 1 trial published in PMC assessed the safety of a 16-week ketogenic diet in patients with recently diagnosed GBM receiving standard-of-care treatment. The primary safety threshold — a 10% weight loss resulting in a BMI below 18.5 in 20% of participants — was not reached, indicating the protocol was safe in this context. Feasibility was assessed by whether patients could maintain blood ketone levels above 0.3 mM for more than 50% of their study days.
Taken together, the clinical picture is this: fasting-based metabolic interventions appear feasible and safe in GBM patients when supervised. Efficacy data from randomized trials are limited and, so far, mixed. Larger and better-designed studies are needed.
Tumor Subtype May Determine Who Responds
Not all GBMs respond equally to fasting. A 2026 study published in Nature Communications found that the efficacy of intermittent fasting in GBM mouse models depended on tumor subtype. IF significantly slowed GBM progression in a Tp53-driven tumor model, while its effect was not significant in the Cdkn2a model. The mechanism involved changes in gut microbiota and altered methionine metabolism that suppressed TGF-β signaling.
This means whether fasting helps may depend partly on the molecular profile of your specific tumor. Understanding markers like TP53 status could eventually help predict who benefits most from metabolic interventions.
Related reading: Understanding Your GBM Molecular Profile: IDH, MGMT, EGFR & Why They Matter
Caloric Restriction: Slightly Different From Fasting
Caloric restriction (CR) is a sustained reduction in total calorie intake — typically 20–40% below baseline — without complete fasting. It shares several mechanisms with IF: lower insulin, lower IGF-1, lower blood glucose. But the two approaches are not identical.
In preclinical glioma models, research from PMC shows that GBM tumor cells are highly dependent on glucose and glutamine, and that restricting these substrates may slow disease progression. Calorie-restricted ketogenic diets reduced tumor growth in high-grade glioma mouse models through effects on angiogenesis, apoptosis, and inflammation.
A registered clinical trial, the ERGO2 trial (NCT01754350) at ClinicalTrials.gov, was specifically designed to test whether restricting glucose availability through calorie restriction and transient fasting could improve the efficacy of re-irradiation in recurrent GBM — applying this preclinical logic directly to human patients.
Preclinical work published in PLOS ONE also suggests that caloric restriction may slow brain tumor growth through multiple molecular mechanisms, including effects on the tumor-promoting inflammation pathway NF-κB. These findings remain at the laboratory stage and require human validation.
Practical Considerations: What Fasting Looks Like During GBM Treatment
For patients actively undergoing treatment, several practical factors shape whether fasting-based approaches are appropriate:
- Corticosteroids and blood sugar: Many GBM patients take dexamethasone to control brain swelling. Steroids raise blood glucose significantly, which may blunt the metabolic benefit of fasting. Discuss steroid management with your team before making dietary changes.
- Nutritional status: GBM and its treatment can cause weight loss, fatigue, and nausea. Aggressive caloric restriction in a malnourished patient is potentially harmful. Feasibility data from clinical trials generally exclude patients with low BMI or poor nutritional status.
- Seizure medications: Some anti-epileptic drugs interact with ketogenic metabolic states. Coordination with your neurology team is important. Related reading: Valproic Acid and Glioblastoma: Can an Anti-Seizure Medication Also Help Fight Your Tumor?
- Timing relative to treatment cycles: Based on DSR research, the most biologically relevant window for short-term fasting is the 24–72 hours surrounding chemotherapy administration. This is also the most studied window in clinical feasibility trials.
- Supervision: All clinical trials that have tested fasting in GBM patients included dietitian support and regular monitoring of glucose, ketones, and body weight. Attempting extended fasting outside a supervised protocol carries real risks.
What the Evidence Does and Does Not Support
It is important to be clear about what the current data shows:
- Supported (mostly preclinical and early-phase human data): Fasting and CR lower circulating glucose, insulin, and IGF-1. These changes may sensitize GBM cells to temozolomide and radiation in animal models. Short-term fasting around chemotherapy appears safe and feasible in cancer patients.
- Not yet supported by randomized trial evidence: That IF or CR extends survival in GBM patients. The ERGO2 trial — the most rigorous randomized human study to date — did not meet its primary survival endpoint.
- Actively under investigation: Optimal fasting duration and timing, the role of tumor molecular subtype in predicting response, and whether repeated fasting cycles during first-line therapy outperform single episodes at recurrence.
The metabolic approach to GBM is scientifically sound. But sound science and proven clinical benefit are not the same thing. Metabolic strategies should be considered adjuncts — not replacements — for surgery, radiation, and temozolomide-based chemotherapy.
Related reading: Integrative Treatments for Glioblastoma: Evidence-Based Complementary Therapies That May Help
The Connection to GBM's Metabolic Resistance
One reason metabolic targeting is attracting serious scientific attention is that GBM's metabolic wiring contributes to treatment resistance. A review in PMC on metabolic reprogramming in GBM notes that GBM reshapes glucose metabolism through the Warburg effect, and that recent evidence points to further rewiring in nucleotide, lipid, and iron metabolism — driving both tumor growth and resistance to radiation and chemotherapy. This means targeting metabolism is not only about reducing fuel for the tumor; it may also help overcome resistance mechanisms.
However, the same review notes that GBM heterogeneity means a metabolic treatment might work for some tumor subtypes but not others. This reinforces the importance of molecular profiling in deciding whether and how metabolic strategies are added to a treatment plan.
When to Talk to Your Doctor
Bring up intermittent fasting or caloric restriction with your neuro-oncologist before making any changes to your eating pattern, especially if you:
- Are currently taking corticosteroids or anti-seizure medications
- Have lost significant weight since diagnosis
- Are in the active chemoradiation phase of treatment
- Have diabetes or another condition that affects glucose regulation
- Are considering an extended fast (beyond 16–24 hours)
Ask specifically about any open metabolic or dietary clinical trials at your center, and request a referral to an oncology-specialized dietitian. Supervised dietary modification as part of a formal protocol is safer and more likely to generate useful data than unsupervised experimentation.
This article is for general information and is not a substitute for medical advice. Always consult your oncologist or care team about your specific situation.