Hyperbaric Oxygen Therapy
How breathing pure oxygen under pressure can help overcome one of glioblastoma's most formidable defenses — low oxygen levels inside the tumor — and make standard treatments more effective.
What Is Hyperbaric Oxygen Therapy?
Hyperbaric oxygen therapy (HBOT) involves breathing 100% pure oxygen while inside a specialized pressurized chamber, typically at 1.5 to 2.5 times normal atmospheric pressure. Under these conditions, your blood plasma can carry up to 10–15 times more dissolved oxygen than it normally does.

100% Oxygen
You breathe pure oxygen instead of the normal 21% found in room air, dramatically increasing oxygen concentration in your blood.
Increased Pressure
The chamber pressure (1.5–2.5 ATA) forces oxygen molecules to dissolve directly into blood plasma, bypassing hemoglobin's normal limits.
Deep Tissue Reach
This super-oxygenated plasma can penetrate areas where red blood cells struggle to go — including the oxygen-starved core of tumors.
The Hypoxia Problem in Glioblastoma
To understand why HBOT matters, you need to understand one of glioblastoma's most dangerous survival tricks: tumor hypoxia.
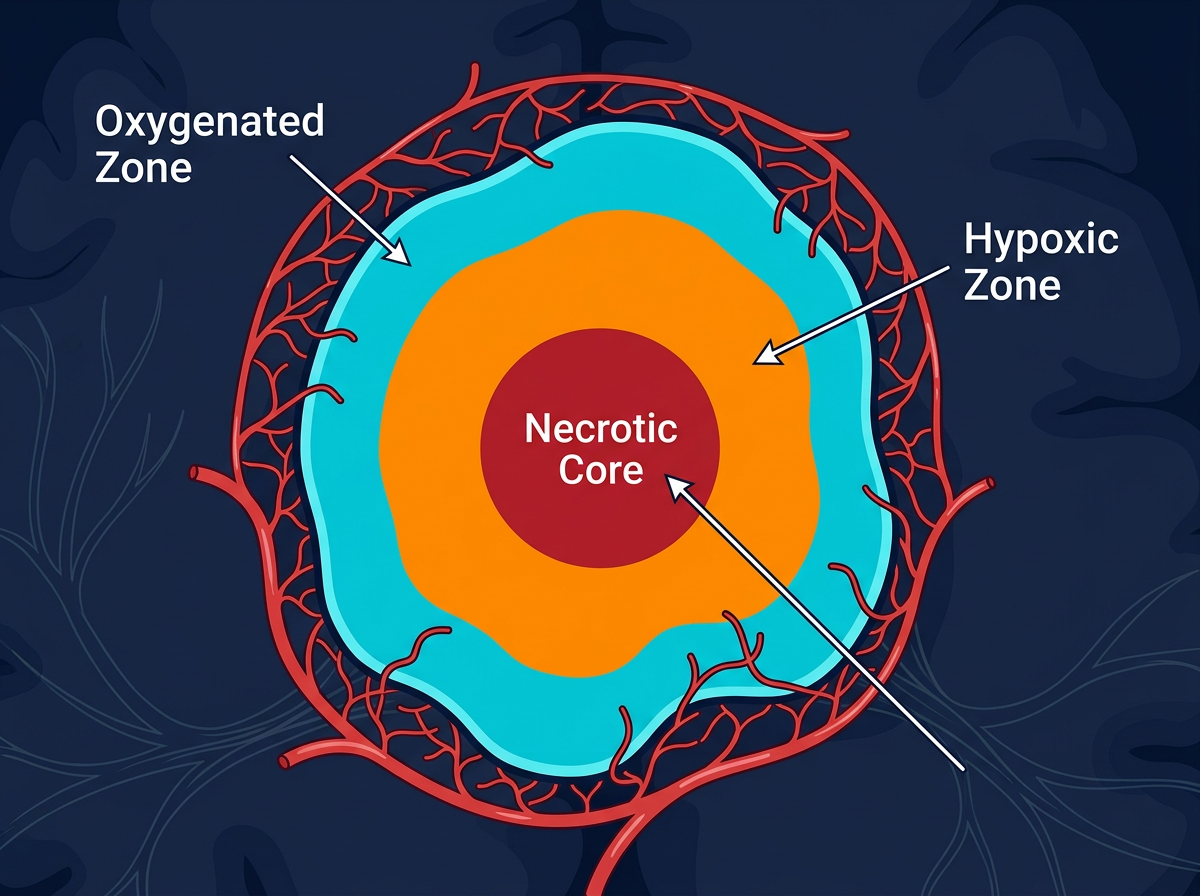
Why Tumors Become Oxygen-Starved
Glioblastoma grows aggressively — so aggressively that it outpaces its own blood supply. The tumor forms new blood vessels (a process called angiogenesis), but these vessels are abnormal, leaky, and disorganized. The result? Large areas within the tumor, especially the core, receive very little oxygen. These are called hypoxic zones.
Why Hypoxia Makes Treatment Harder
- Radiation resistance: Radiation works by generating reactive oxygen species (ROS) that damage tumor DNA. Without oxygen, this process is up to 2–3× less effective. This is known as the "oxygen enhancement ratio."
- Chemotherapy resistance: Temozolomide and other drugs rely on adequate blood flow to reach tumor cells. Hypoxic regions with poor blood supply receive lower drug concentrations.
- Tumor aggression: Hypoxia activates a protein called HIF-1α (hypoxia-inducible factor), which triggers genes that promote tumor invasion, stem cell maintenance, and resistance to cell death.
In simple terms: Low oxygen in the tumor acts like a shield — it protects cancer cells from the very treatments designed to kill them. HBOT aims to remove that shield.
How HBOT Helps Fight Glioblastoma
HBOT doesn't kill cancer cells on its own — instead, it works as a treatment enhancer (a "sensitizer") that makes other therapies more effective through several mechanisms.
Radiation Sensitization
Radiation kills cancer cells primarily by creating free radicals — highly reactive oxygen molecules that shatter tumor DNA. When oxygen levels are low, fewer free radicals form, and the DNA damage is more easily repaired by the cancer cell. By flooding the tumor with oxygen before radiation, HBOT increases the production of these free radicals, making each radiation session significantly more destructive to cancer cells. Research shows that oxygenated tumor cells can be 2–3 times more sensitive to radiation than hypoxic ones.
Improved Chemotherapy Delivery
Temozolomide (TMZ) — the standard chemotherapy for glioblastoma — must physically reach the tumor cells to work. HBOT temporarily normalizes blood flow in and around the tumor, allowing more drug molecules to penetrate deeper into tumor tissue. Some preclinical studies suggest HBOT may also make the blood-brain barrier slightly more permeable, potentially improving drug access to the brain.
Suppressing HIF-1α Signaling
When tumor cells detect low oxygen, they activate HIF-1α — a master regulator protein that switches on survival programs. These programs promote new (abnormal) blood vessel growth, increase tumor cell migration into healthy brain tissue, and help maintain the cancer stem cell population that drives recurrence. By restoring oxygen levels, HBOT can reduce HIF-1α activity, potentially slowing these aggressive tumor behaviors.
Immune System Support
Immune cells — particularly macrophages and T-cells — require adequate oxygen to function properly. In hypoxic tumor environments, immune surveillance is suppressed. HBOT can help restore immune cell activity within the tumor microenvironment, potentially improving the body's natural ability to recognize and attack cancer cells. This is especially relevant as immunotherapy approaches for glioblastoma continue to develop.
Reducing Radiation-Induced Brain Injury
Paradoxically, HBOT may also help protect healthy brain tissue. Radiation necrosis — damage to normal brain tissue caused by radiation treatment — is a known side effect. HBOT has been studied and used clinically to treat radiation necrosis, as the increased oxygen promotes healing and new blood vessel growth in damaged healthy tissue. Some neuro-oncologists consider HBOT an established treatment for this particular complication.
What Does the Clinical Evidence Say?
While HBOT is not yet part of the standard-of-care protocol for glioblastoma, a growing body of clinical and preclinical research supports its potential.
Radiation + HBOT Studies
Several clinical studies from the 1970s–2000s showed improved tumor control when HBOT was administered before radiation sessions. A 2012 Cochrane review noted trends toward improved local tumor control, though more randomized trials are needed.
HBOT + Temozolomide
Preclinical studies in animal glioma models have shown that combining HBOT with temozolomide can reduce tumor volume more than either treatment alone. Pilot human studies are underway at several centers.
HBOT for Radiation Necrosis
This is the most established use of HBOT in brain cancer patients. Multiple retrospective studies and case series have documented clinical improvement in patients with symptomatic radiation necrosis who underwent HBOT, with response rates ranging from 50–100% across different studies.
HBOT + Ketogenic Diet (Metabolic Approach)
Dr. Dominic D'Agostino's research at the University of South Florida has explored combining HBOT with a ketogenic diet in glioma models. The combination reduced tumor growth and extended survival in preclinical models by attacking cancer metabolism from two angles — restricting glucose while flooding tumors with toxic levels of oxygen.
What to Expect During HBOT
Session Duration
Each session lasts 60–90 minutes. You lie comfortably inside the chamber while breathing normally.
Pressure Level
The chamber is pressurized to 1.5–2.5 ATA (atmospheres absolute). You may feel pressure in your ears — similar to an airplane — which can be relieved by swallowing or yawning.
Frequency
A typical protocol involves 20–40 sessions, usually once daily on weekdays. When combined with radiation, HBOT is often given 30–60 minutes before each radiation session.
Comfort
Modern monoplace chambers have clear walls so you can see outside. Many patients read, watch videos, or rest during sessions. You can communicate with the technician at all times.
Safety & Side Effects
HBOT is generally well-tolerated, but like any medical treatment, it has potential side effects that patients should be aware of.
Common & Mild
- • Ear pressure or mild discomfort (barotrauma) — usually preventable with equalization techniques
- • Temporary nearsightedness (myopia) — typically reverses after treatment ends
- • Fatigue after sessions
- • Lightheadedness
Rare but Serious
- • Oxygen toxicity seizures (very rare at standard clinical pressures, <0.1%)
- • Pneumothorax (collapsed lung) — extremely rare
- • Sinus pain if sinuses are congested
- • Not recommended with certain chemotherapy agents (bleomycin) — discuss with your oncologist
Questions to Ask Your Neuro-Oncologist
If you're considering HBOT as part of your treatment plan, here are evidence-informed questions to guide your conversation.
Could HBOT be timed with my radiation sessions to improve their effectiveness?
Is my tumor showing signs of hypoxia on imaging that might make me a good candidate for HBOT?
Are there any interactions between HBOT and my current medications, including temozolomide or bevacizumab?
Would you recommend HBOT as a treatment for radiation necrosis if it develops?
Are there any clinical trials combining HBOT with my treatment protocol that I might be eligible for?
Is there a reputable HBOT center near my treatment facility that your team has worked with before?
The Bottom Line
Hyperbaric oxygen therapy is not a standalone cure for glioblastoma. However, growing evidence suggests it can serve as a meaningful adjunct therapy — enhancing radiation effectiveness, improving chemotherapy delivery, supporting immune function, and treating radiation-induced brain injury.
As our understanding of the tumor microenvironment deepens, HBOT's role in addressing hypoxia-driven resistance is becoming harder to ignore. Discuss it with your neuro-oncology team to determine whether it may be appropriate for your individual situation.
Medical Disclaimer: This content is for educational purposes only and should not replace professional medical advice. Always consult your neuro-oncology team before making treatment decisions.