Why Recurrent GBM Is So Hard to Treat
Glioblastoma is one of the most aggressive brain tumors known. Even after surgery, radiation, and chemotherapy, it almost always comes back. When it does, options narrow fast. Standard external-beam radiation is rarely repeated because nearby brain tissue has already received close to its safe dose limit. Chemotherapy choices are limited. Bevacizumab can slow swelling but does not reliably extend life. For many patients, the search for a new approach begins at first recurrence.
That search has brought researchers and patients to a decades-old idea with a modern update: Boron Neutron Capture Therapy, or BNCT. The concept is precise in a way standard radiation cannot match — it targets individual tumor cells while aiming to leave healthy tissue alone. This article explains how BNCT works, what clinical data shows for recurrent GBM, who might be a candidate, and what questions to bring to your oncology team.
For broader context on why GBM comes back and what the overall salvage landscape looks like, see our guide on recurrent GBM: why it comes back, what you can do, and how to navigate what comes next.
What Is BNCT? The Two-Step Mechanism
BNCT is a form of targeted radiotherapy that works in two steps. Understanding both is key to seeing why this approach may be useful for a tumor as infiltrative as GBM.
Step 1: Delivering the Boron
A boron-containing drug — most commonly boronophenylalanine (BPA) — is given intravenously. BPA is structurally similar to the amino acid phenylalanine. Because rapidly dividing tumor cells consume amino acids at a high rate, they absorb BPA preferentially. Research published in PMC shows that the boron compound is selectively taken up by malignant tumor cells, while nearby normal brain cells accumulate far less of it.
Step 2: Neutron Irradiation
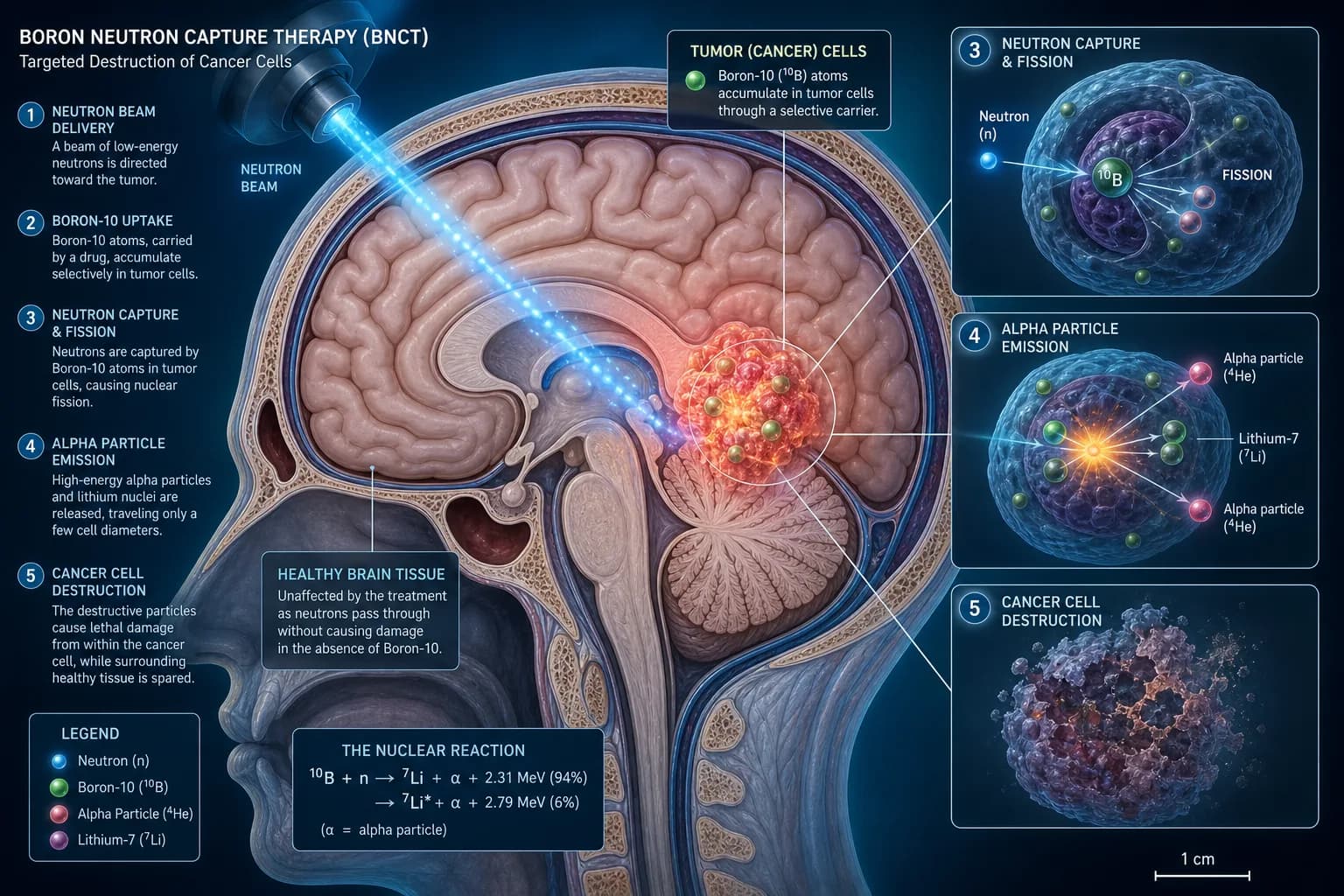
Once enough boron has concentrated inside the tumor cells, the treatment area is exposed to a beam of low-energy neutrons. By exploiting the ¹⁰B(n,α)⁷Li nuclear reaction, BNCT enables precise eradication of boron-loaded tumor cells while sparing adjacent healthy tissues — a feature described as particularly useful for invasive or radioresistant recurrent tumors.
Neutrons alone cause relatively little harm to tissue. But when a neutron is captured by a boron-10 atom inside a tumor cell, a small nuclear fission event occurs, releasing two high-energy particles: an alpha particle and a lithium-7 nucleus. These particles travel only a few micrometers — roughly the diameter of a cell — releasing their energy directly within the cancer cell where the boron was concentrated. The result is irreversible DNA damage and cell death, confined almost entirely to the cell that held the boron.
This sub-cellular precision is what separates BNCT from conventional external-beam radiation, which cannot distinguish between tumor cells and healthy neurons at that scale.
A Brief History: From Reactor Halls to Hospital Accelerators
BNCT is not new. The concept was first proposed in 1936 and applied clinically for GBM as early as 1951. Early U.S. trials used nuclear reactors as neutron sources and produced disappointing results, largely because boron-delivery drugs were inadequate and thermal neutrons from reactors had limited depth penetration. U.S. clinical trials were eventually suspended.
Two advances changed the field. Better boron carriers — especially BPA — were developed. And modern accelerator-based neutron systems, improved boron delivery agents, and imaging techniques such as PET and MRI now allow clinicians to better select patients and personalize treatment.
Accelerator-based BNCT (AB-BNCT) uses a compact cyclotron to generate neutrons inside a hospital building, with no nuclear reactor required. This makes the technology far more accessible. Japan moved first: in 2020, an accelerator-based BNCT system received regulatory approval there for unresectable locally recurrent head and neck cancers, with brain tumor indications under active investigation. Clinical programs are now running across Asia, Europe, and several other regions.
What the Clinical Data Shows for Recurrent GBM
BNCT data for recurrent GBM comes primarily from Japan, Finland, Taiwan, and South Korea. The trials are mostly small Phase I and Phase II studies, so results should be interpreted carefully. Still, the signals are notable given how difficult recurrent GBM is to treat.
The JG002 Phase II Trial
One of the most cited studies is the JG002 multicenter Phase II trial, which enrolled 27 patients with recurrent malignant glioma — 24 with GBM — using an accelerator-based cyclotron system and BPA as the boron carrier. All patients had already received standard radiation therapy. The results showed markedly excellent clinical results, with a median overall survival of 18.9 months after treating recurrent glioblastoma. The trial also found that brain edema — a known risk of re-irradiation — could be managed with bevacizumab.
An extended follow-up of this trial, published in 2025, further examined long-term outcomes. The analysis reported a median survival of 19.2 months in recurrent glioblastoma patients post-BNCT, with some patients surviving beyond two years — an uncommon outcome in this population.
The Phase 1 Dose-Escalation Trial (NCT05737212)
A more recent multicenter Phase 1 study enrolled patients with recurrent high-grade gliomas, mostly GBMs, to evaluate safety and pharmacokinetics across different radiation dose levels. This study demonstrated an acceptable safety profile of BNCT and suggests potential survival benefits in recurrent high-grade glioma, though the authors noted that extended observation is still needed to confirm long-term efficacy.
The full protocol and eligibility criteria for this trial are registered at ClinicalTrials.gov (NCT05737212).
What These Numbers Mean
Median survival for recurrent GBM after standard second-line therapy typically falls in the range of 6 to 9 months for most systemic options. Numbers in the 18–19-month range from BNCT trials stand out. But these are small, non-randomized studies without matched control arms in most cases. They do not prove that BNCT extends survival compared to other approaches. What they do suggest is that BNCT appears safe in this setting and may be worth studying in larger randomized trials.
Your tumor's molecular profile — including IDH status and MGMT methylation — is critical context when weighing any salvage option. See our deep dive on understanding your GBM molecular profile: IDH, MGMT, EGFR, and why they matter.
The BPA-PET Scan: A Personalized Eligibility Test
Not every patient with recurrent GBM will be a BNCT candidate. One of the most important pre-treatment steps is a specialized PET scan using a radioactive form of BPA (¹⁸F-BPA-PET). This scan measures how well BPA accumulates inside the tumor cells relative to normal tissue.
¹⁸F-BPA injection holds the potential to ascertain BPA concentration within the tumor, enabling meticulous treatment planning and outcome evaluation, based on tumor-to-normal tissue ratios. If the ratio is too low — meaning BPA does not concentrate enough in the tumor — BNCT is unlikely to work well for that patient. This PET scan acts as a precision filter, and it is one of the features that makes BNCT genuinely personalized rather than applied uniformly.
Clinicians also use this imaging to guide dosimetry — calculating how much neutron radiation can safely be delivered to achieve the needed effect inside the tumor without exceeding safe limits in surrounding brain tissue.
Who May Be a Candidate for BNCT?
Eligibility criteria vary by trial and institution, but the following factors appear consistently in published protocols and ongoing studies:
- Confirmed recurrent GBM (IDH-wildtype, WHO Grade 4 per 2021 WHO classification) with radiographic progression confirmed by MRI or functional imaging
- Prior standard radiotherapy — BNCT is being studied specifically as a re-irradiation strategy for patients who have already received standard-of-care radiation (typically 54–66 Gy)
- Adequate performance status — most trials require a Karnofsky Performance Score (KPS) of at least 60, meaning the patient can perform self-care activities
- Adequate organ function, including acceptable kidney, liver, and bone marrow laboratory values
- No metal implants (such as pacemakers) that would interfere with treatment delivery
- Favorable BPA-PET result — sufficient tumor uptake of the boron carrier on pre-treatment imaging
- Ability to lie still during the treatment session, which can last 30 minutes to one hour in the neutron beam
Patients who are bevacizumab-naive appear to have been prioritized in some studies. However, protocols are evolving as data matures. Always verify current eligibility requirements directly with the treating center or on ClinicalTrials.gov.
Potential Risks and Side Effects
Like all forms of radiation therapy, BNCT carries risks. The most clinically relevant for recurrent GBM patients include:
- Brain edema (swelling). Re-irradiation of any kind can worsen swelling in and around the tumor. Trial data from JG002 noted this risk but found it could be managed with bevacizumab. Steroids may also be used to control inflammation.
- Radiation necrosis. A delayed injury to normal brain tissue, sometimes difficult to distinguish from tumor regrowth on standard MRI. This is a known complication of any brain re-irradiation strategy, not unique to BNCT.
- Skin and scalp effects. Depending on tumor location relative to the surface of the head, local skin reactions are possible.
- Fatigue. Common after any type of radiation therapy.
- Depth limitations. Neutron beams lose intensity with depth. Tumors located very deep in the brain receive lower neutron fluence, which may affect treatment efficacy. This is a known technical limitation of the current approach.
Because BNCT is still investigational for GBM in most countries, its full long-term toxicity profile is still being established. Participation in a clinical trial provides the most structured monitoring for these effects.
Access and Availability: Where Is BNCT Available?
BNCT for GBM is currently available primarily through clinical trials. Outside Japan — where it is approved for recurrent head and neck cancers and brain tumor trials are ongoing — access is limited to research centers with accelerator-based neutron sources.
Active BNCT programs for brain tumors are operating or in development in Japan, South Korea, Finland, Taiwan, Israel, Argentina, and parts of Europe. In the United States, BNCT for GBM is not yet FDA-approved, but U.S. patients may qualify for international trials or compassionate-use pathways. Search for open studies at ClinicalTrials.gov using the terms "boron neutron capture therapy glioblastoma."
The technology continues to advance. Researchers are studying new boron-delivery agents — including boron-containing nanoparticles that may be paired with tumor-targeting antibodies or peptides — to improve selectivity and penetration through the blood-brain barrier. These next-generation carriers remain in preclinical and early clinical development.
BNCT is part of a broader wave of emerging precision radiation and targeted strategies for GBM. For a look at other novel approaches in this space, see our article on sonodynamic therapy, gene therapy, and emerging platforms in GBM.
How BNCT Fits Into a Broader Recurrence Strategy
BNCT should not be framed as a replacement for standard-of-care management. At recurrence, current evidence-based options include bevacizumab, tumor-treating fields (TTFields), re-resection where feasible, temozolomide rechallenge in select molecular profiles, and enrollment in clinical trials.
BNCT fits best as a re-irradiation option for patients who have already exhausted conventional re-irradiation or are not candidates for it. It is most compelling within a clinical trial, where patients receive structured monitoring, imaging follow-up, and access to a multidisciplinary team managing both efficacy and toxicity.
Other precision approaches — including immunotherapy strategies and novel targeted agents — are also being studied in parallel. For a comprehensive view of the immunotherapy landscape at recurrence, see our article on the immunotherapy landscape in GBM: beyond checkpoint inhibitors.
Metabolic and integrative strategies may complement any radiation-based therapy and are worth discussing with your team. Our overview of integrative treatments for glioblastoma covers complementary options that have evidence supporting their evaluation alongside standard approaches.
The Bottom Line on BNCT for Recurrent GBM
BNCT is a cell-selective form of radiation therapy with meaningful early signals in recurrent GBM — a disease setting where options are genuinely limited. Phase II data from Japan suggests median survival in the 18–19-month range for carefully selected patients, though these figures come from small, non-randomized studies and should be interpreted with caution.
The approach is not yet standard of care for GBM anywhere in the world and remains investigational globally. Access is currently tied to clinical trial participation or specialized centers. For patients with documented recurrence who have already received standard radiation, BNCT is a scientifically grounded precision option worth raising with your neuro-oncologist — particularly if you are near a center running an active BNCT trial.
When to Talk to Your Doctor
Bring up BNCT with your neuro-oncologist or radiation oncologist if:
- Your GBM has recurred after standard chemoradiation and you are exploring re-irradiation options
- Conventional repeat radiation has been ruled out due to prior dose exposure
- You are interested in clinical trial options beyond bevacizumab or temozolomide rechallenge
- You are near a center running an active BNCT program
Ask your team whether a ¹⁸F-BPA-PET scan is available to assess your tumor's boron uptake, and whether any active BNCT trials for GBM are accepting patients at their center or at affiliated institutions.
This article is for general information and is not a substitute for medical advice. Always consult your oncologist or care team about your specific situation.