Sustained tumor regression with 2-DG after progression on standard chemoradiotherapy
A 40-year-old woman from the United Kingdom with H3 K27-altered diffuse midline glioma, WHO grade 4, presented after progression on standard therapy with severe neurological decline, high steroid burden, and a Karnofsky Performance Status of approximately 40.
Tumor response
Partial regression
Serial MRI showed progressive shrinkage over 11 months with resolution of mass effect.
Functional recovery
KPS 40 → 70
She regained walking, speech, coordination, and independence in daily activity.
Steroid reduction
8 mg → 1 mg
Dexamethasone was tapered by 87.5%, improving quality of life substantially.
Treatment exposure
30 cycles / 11 months
Intravenous 2-DG was delivered with close monitoring and no reported adverse events.
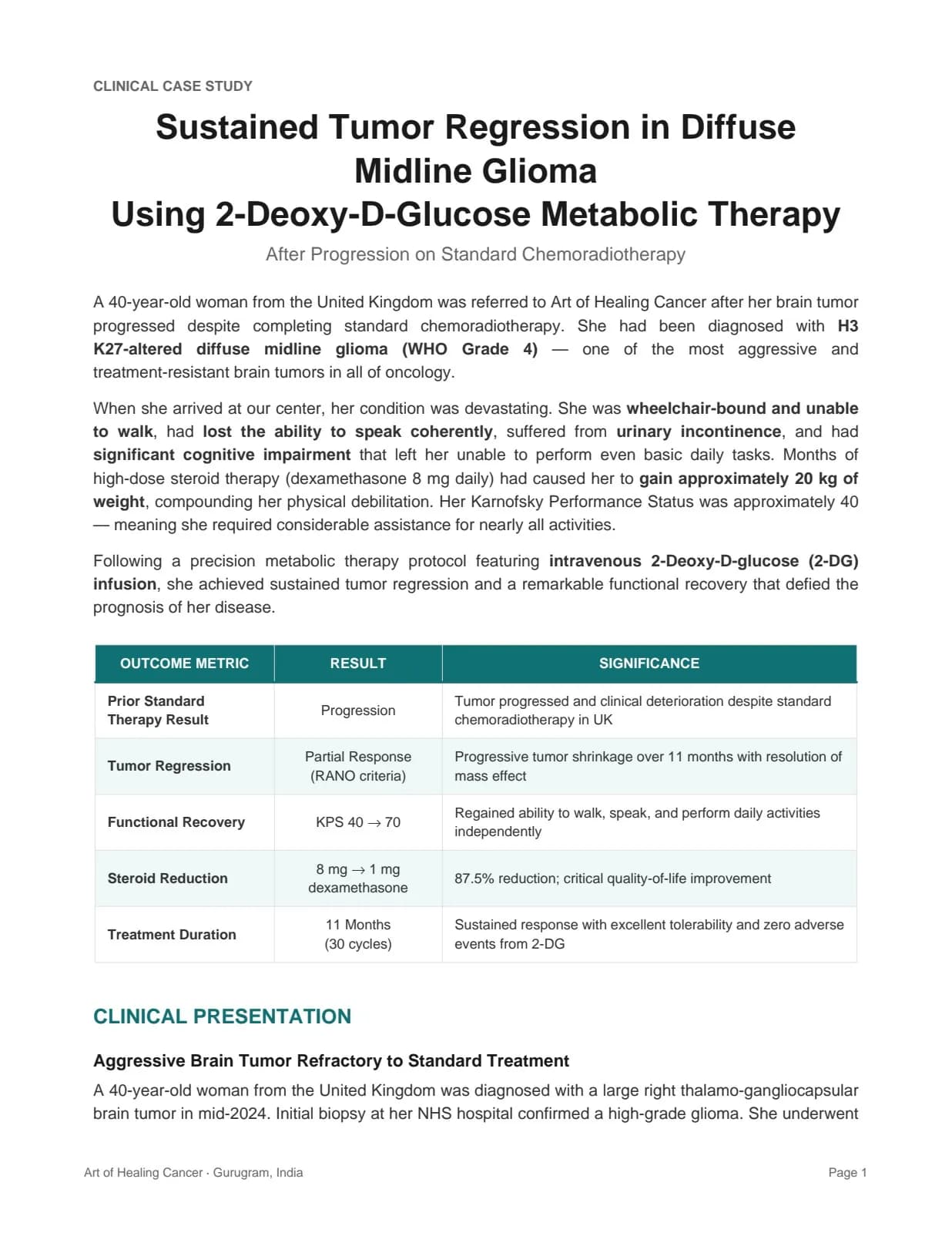
Clinical baseline
At referral, the tumor measured 4.8 × 4.5 × 4.6 cm with 8.9 mm midline shift. She was wheelchair-bound, unable to walk, had impaired speech, urinary incontinence, cognitive dysfunction, and severe steroid-related debility after prolonged dexamethasone 8 mg daily.
Why this case matters
H3 K27-altered diffuse midline glioma is among the most lethal malignancies in oncology, with few effective options after radiation failure. This report is notable for radiographic regression, and also for durable functional recovery, loss of midline shift, steroid taper, and preserved tolerability through a precision metabolic regimen.
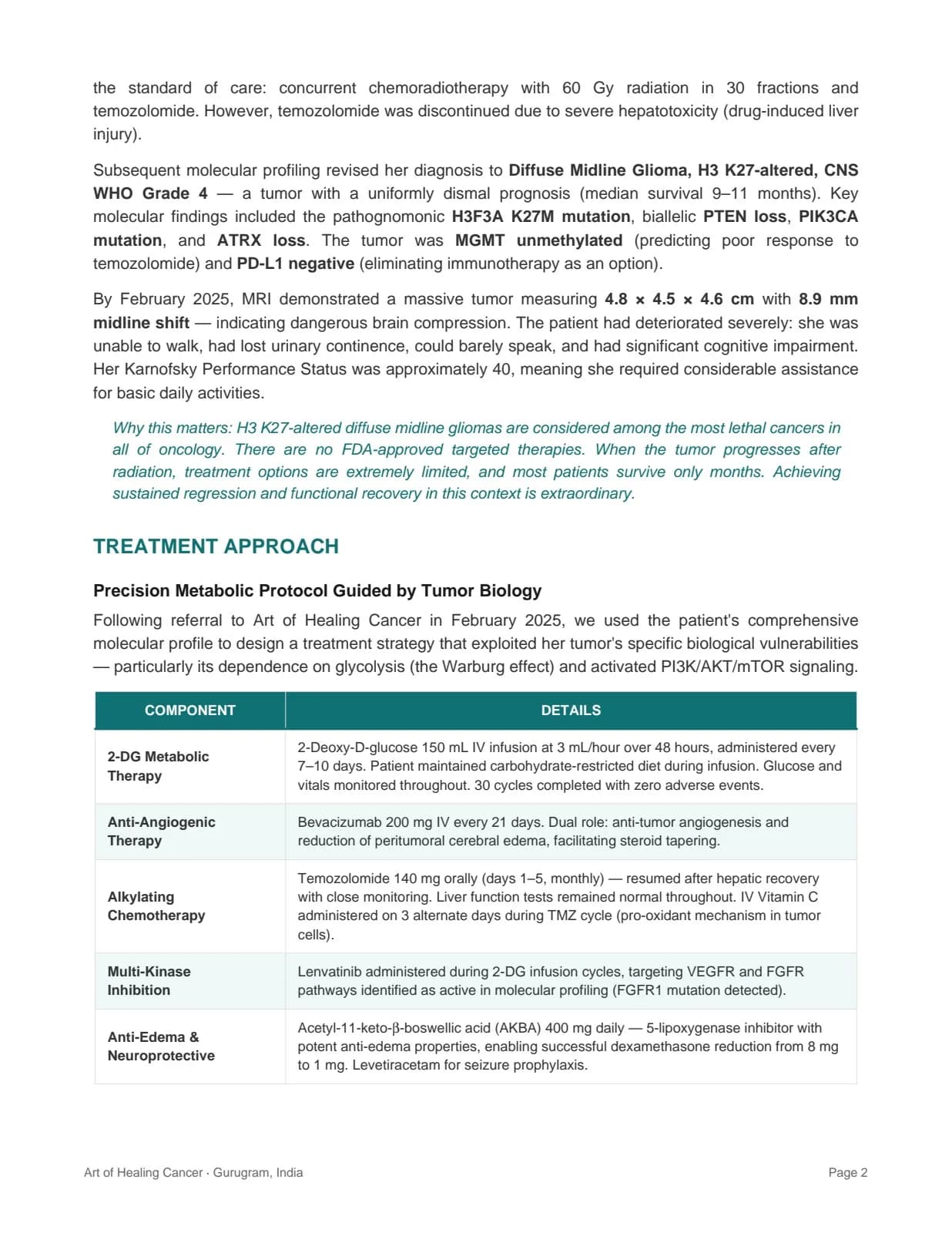
Precision treatment architecture
2-DG metabolic therapy
150 mL IV infusion at 3 mL/hour over 48 hours every 7–10 days with carbohydrate restriction and glucose monitoring.
Bevacizumab support
Anti-angiogenic therapy used for tumor control and edema reduction to support steroid tapering.
Temozolomide reintroduction
Restarted after hepatic recovery with close liver monitoring and IV vitamin C support during cycles.
Lenvatinib targeting
Added during infusion cycles to address active VEGFR/FGFR signaling identified on profiling.
Adjunct biologic stack
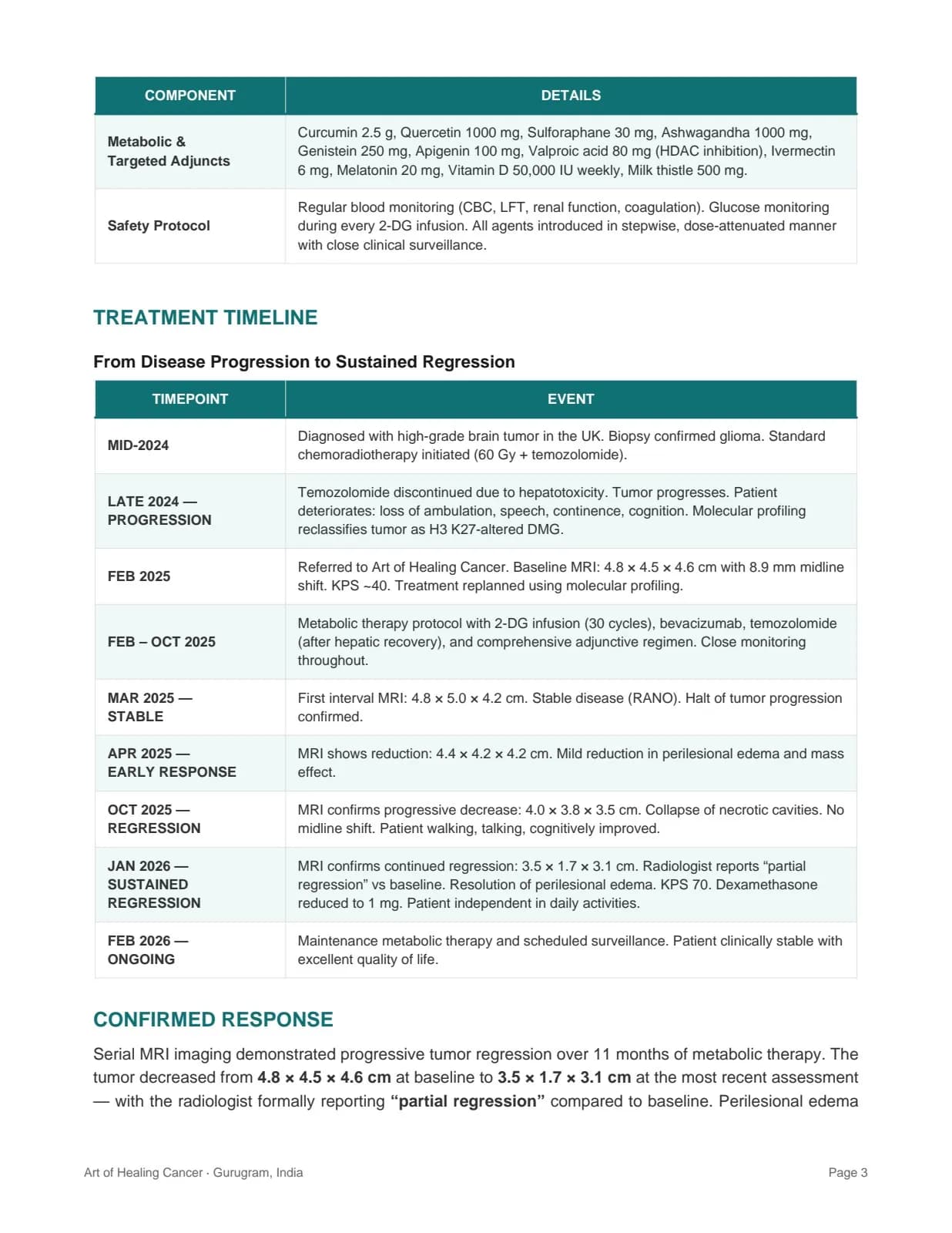
Included AKBA, curcumin, quercetin, sulforaphane, melatonin, vitamin D, valproic acid, ivermectin, and other supportive agents.
Safety protocol
CBC, liver, renal, coagulation, glucose, and vitals were monitored continuously through a stepwise protocol.
Timeline of regression and recovery
Mid-2024
Diagnosis and first-line treatment
Large right thalamo-gangliocapsular tumor diagnosed in the UK; standard chemoradiotherapy initiated with 60 Gy and temozolomide.
Late 2024
Progression after standard therapy
Temozolomide stopped due to hepatotoxicity; disease progressed with loss of ambulation, continence, speech, and cognition.
Feb 2025
Referral and biological re-planning
Molecular profiling confirmed H3 K27-altered diffuse midline glioma with baseline MRI at 4.8 × 4.5 × 4.6 cm and 8.9 mm midline shift.
Mar–Apr 2025
Stability then early response
Initial MRI confirmed disease stabilization, followed by measurable size reduction and reduced edema.
Oct 2025
Clear regression
MRI showed 4.0 × 3.8 × 3.5 cm, collapse of necrotic cavities, and resolution of midline shift as function improved.
Jan–Feb 2026
Sustained regression
MRI reduced further to 3.5 × 1.7 × 3.1 cm, with KPS 70, steroid taper to 1 mg, and ongoing maintenance.
Clinical significance
Metabolic vulnerability as a target: the biology suggested deep glycolytic dependence and PI3K/AKT/mTOR activation, making 2-DG a rational metabolic intervention in a tumor with no meaningful remaining standard options.
Multimodal precision: the regimen combined metabolic therapy, anti-angiogenic support, alkylating chemotherapy, multi-kinase inhibition, and adjunct biologic modulation selected from molecular profiling rather than generic protocol repetition.
Durability and function: across five serial MRI assessments, the response deepened while the patient regained ambulation, speech, coordination, seizure control, and day-to-day independence.
Case 1 video testimonial
A first-person testimonial can support the clinical report once hosted through a video platform or Cloud Storage.
Video hosting needed
The original 193 MB video was removed from the codebase because GitHub only accepts files up to 100 MB.
Placement note
Add the hosted video URL here later to restore the embedded testimonial without adding a large file to GitHub.
Report scans, charts, and imaging pages