Treating Glioblastoma Demands More Than a Protocol - It Demands Intelligence
A smarter, more adaptive philosophy for glioblastoma care - one that deploys every available tool with precision, creativity, and purpose.
The problem with "standard"
Glioblastoma is not a standard cancer. It is the most aggressive primary brain tumor, with a biology that adapts, resists, and evolves. It crosses boundaries that other cancers don't. It hides behind the blood-brain barrier. It infiltrates healthy tissue in ways that make clean surgical margins almost impossible. And it has a remarkable capacity to develop resistance to the very therapies designed to destroy it.
So why do most treatment plans look the same regardless of the tumor?
The standard-of-care for glioblastoma - surgery, radiation, and temozolomide, known as the Stupp protocol - was established in 2005. It remains the foundation, and it matters. But in twenty years, median survival has moved only modestly. For too many patients, the conversation ends where the protocol ends.
We believe the conversation should be just beginning.
This is why we advocate for something different: an Intelligence Layer - a philosophy of treatment that sits above any single drug, any single protocol, any single modality. It is the commitment to think harder, look wider, adapt faster, and never stop asking: what else can we do?
What is the intelligence layer?
Think of the Intelligence Layer not as a specific treatment plan, but as the operating system that drives every treatment decision.
It is the difference between following a recipe and truly understanding cooking - between executing steps and understanding why each step matters, when to deviate, and how to adapt when the ingredients change.
In glioblastoma care, the Intelligence Layer means:
- Seeing the full range of available treatments - the first-line options, and the second, third, and tenth options that exist across oncology, across medicine, across the world.
- Understanding the tumor's biology at a molecular level - its mutations, its pathways, its vulnerabilities - and matching treatments to that biology, not to a generic protocol.
- Monitoring and adapting in real time, because glioblastoma evolves, and the treatment strategy must evolve with it.
- Balancing efficacy with quality of life, because extending survival means nothing if the patient cannot live during that time.
- Drawing from every discipline - oncology, neurosurgery, radiology, metabolic medicine, immunology, integrative medicine - to build a treatment approach as multifaceted as the disease itself.
The Intelligence Layer is what transforms a treatment protocol into a treatment strategy. And that strategy rests on four foundational pillars.
The four pillars
Every tool in the arsenal

Glioblastoma does not fight with one weapon. Neither should we. The first pillar is the conviction that no single modality is sufficient, and no legitimate modality should be dismissed. The most effective strategies draw from every available category of intervention - combining them thoughtfully, sequencing them strategically, and tailoring them to the individual patient's tumor biology.
The power of repurposing

Some of the most promising tools in the fight against glioblastoma were never designed for it. Drug repurposing - taking medications approved for other conditions and applying them to glioblastoma - is one of the most exciting and practically important strategies in modern oncology.
Biology doesn't respect disease labels. The molecular pathways that drive glioblastoma - PI3K/AKT/mTOR, EGFR signaling, angiogenesis - appear across many diseases. A drug that blocks a pathway in breast cancer may block the same pathway in glioblastoma.
The right dose, not the maximum dose

For decades, the dominant philosophy in cancer chemotherapy has been maximum tolerated dose (MTD): give the highest dose the patient can physically withstand. In practice, for glioblastoma, it often creates a painful paradox: the treatment becomes so toxic that patients can't sustain it long enough for it to work.
The Intelligence Layer embraces a different philosophy: the right dose is the dose that achieves the therapeutic goal while preserving the patient's ability to live, function, and continue treatment.
The art of treating cancer

Medicine is both a science and an art. Nowhere is this truer than in glioblastoma. The first three pillars are about what we deploy and how we dose it. The fourth pillar is about something harder to quantify: the judgment, creativity, timing, and human wisdom that determines how all the pieces come together.
How the intelligence layer works in practice
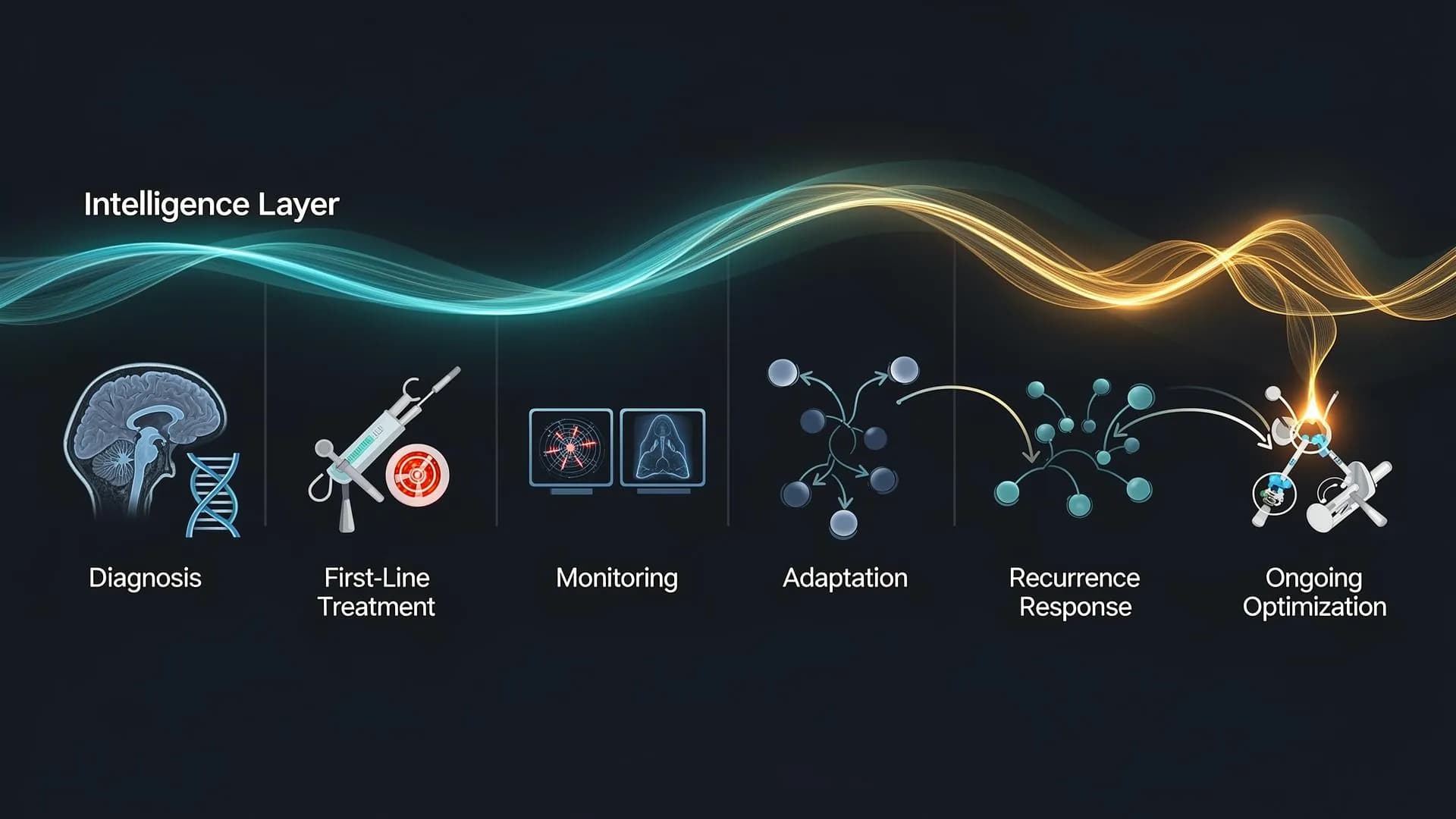
At diagnosis
Comprehensive molecular profiling (IDH status, MGMT methylation, EGFR amplification, full genomic sequencing) to understand the tumor's specific biology and identify targetable vulnerabilities from day one.
During first-line treatment
Standard-of-care forms the foundation - but the Intelligence Layer asks: Can we add TTFields? Should we adjust TMZ dosing based on MGMT status? Are there clinical trials alongside standard therapy?
At every decision point
Regular reassessment using advanced imaging and liquid biopsy monitoring. Treatment adjustments based on how the tumor is actually responding, not just on a predetermined schedule.
At recurrence
When first-line treatment fails, the protocol often runs out of answers. The Intelligence Layer doesn't. It draws from the full spectrum - repurposed agents, immunotherapy trials, metronomic dosing, metabolic interventions, Y-90 radioembolization.
Throughout treatment
Continuous work on supportive care, side effect management, quality of life, and helping the patient stay in charge of decisions. The goal is not survival counted in days; it is survival lived.
Glioblastoma is a formidable adversary. We do not minimize that. But we also refuse to accept that the tools available today represent the limits of what can be done.
The Intelligence Layer is our answer to a disease that demands more than standard thinking. It is the commitment to deploy every available tool, to look beyond the boundaries of neuro-oncology into the wider world of medicine for answers, to dose with wisdom rather than brute force, and to bring the full art of medicine to bear on every treatment decision.
This is not about false hope. It is about informed hope. You deserve nothing less.